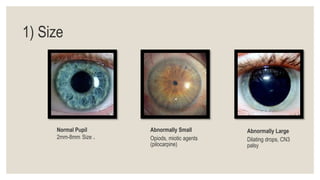
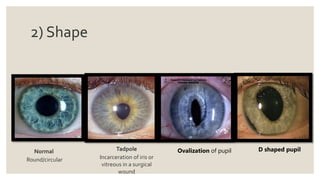
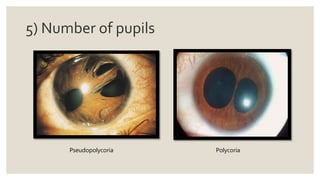
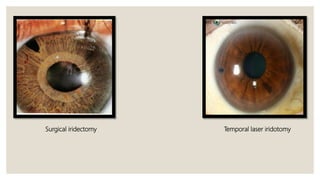
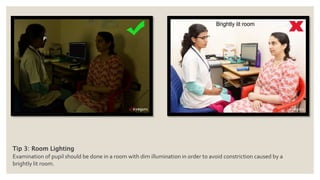
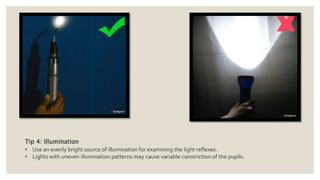
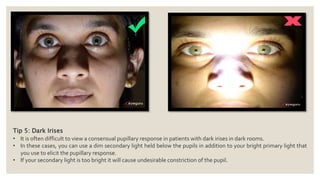
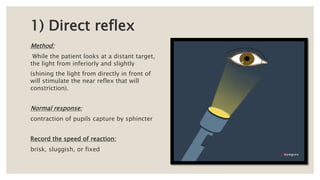
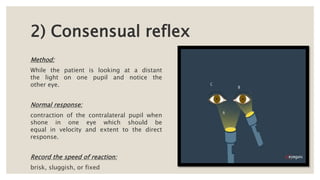
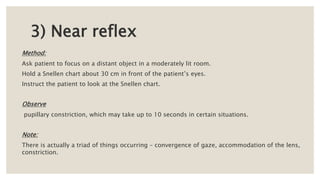
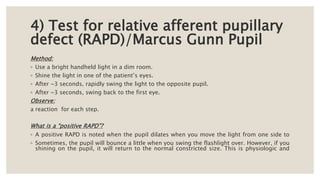
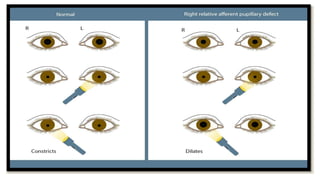
This document provides guidance on examining the pupil, including what aspects to examine (size, shape, position, color, symmetry, number), tips for the examination (seating position, fixation, lighting, dark irises), and how to examine pupil reflexes (direct reflex, consensual reflex, near reflex, relative afferent pupillary defect test). Key items that should be examined include size, shape, position, color, and symmetry of the pupils. The tips recommend dim lighting, having the patient fixate on a distant target, and using a secondary light for patients with dark irises. Pupillary reflexes should be tested via direct and consensual response, near reflex, and relative afferent pupillary