Downloaded 1,490 times



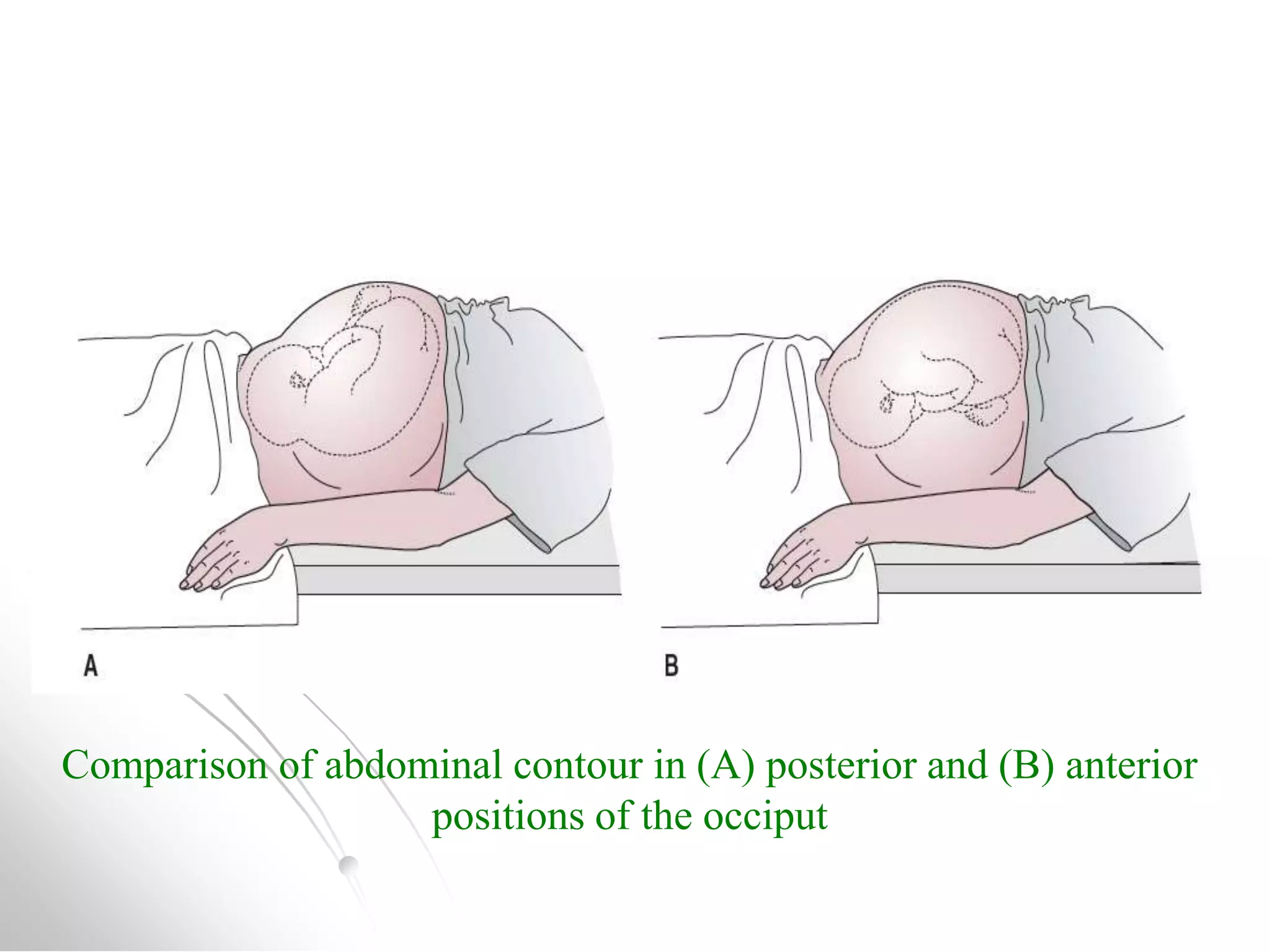


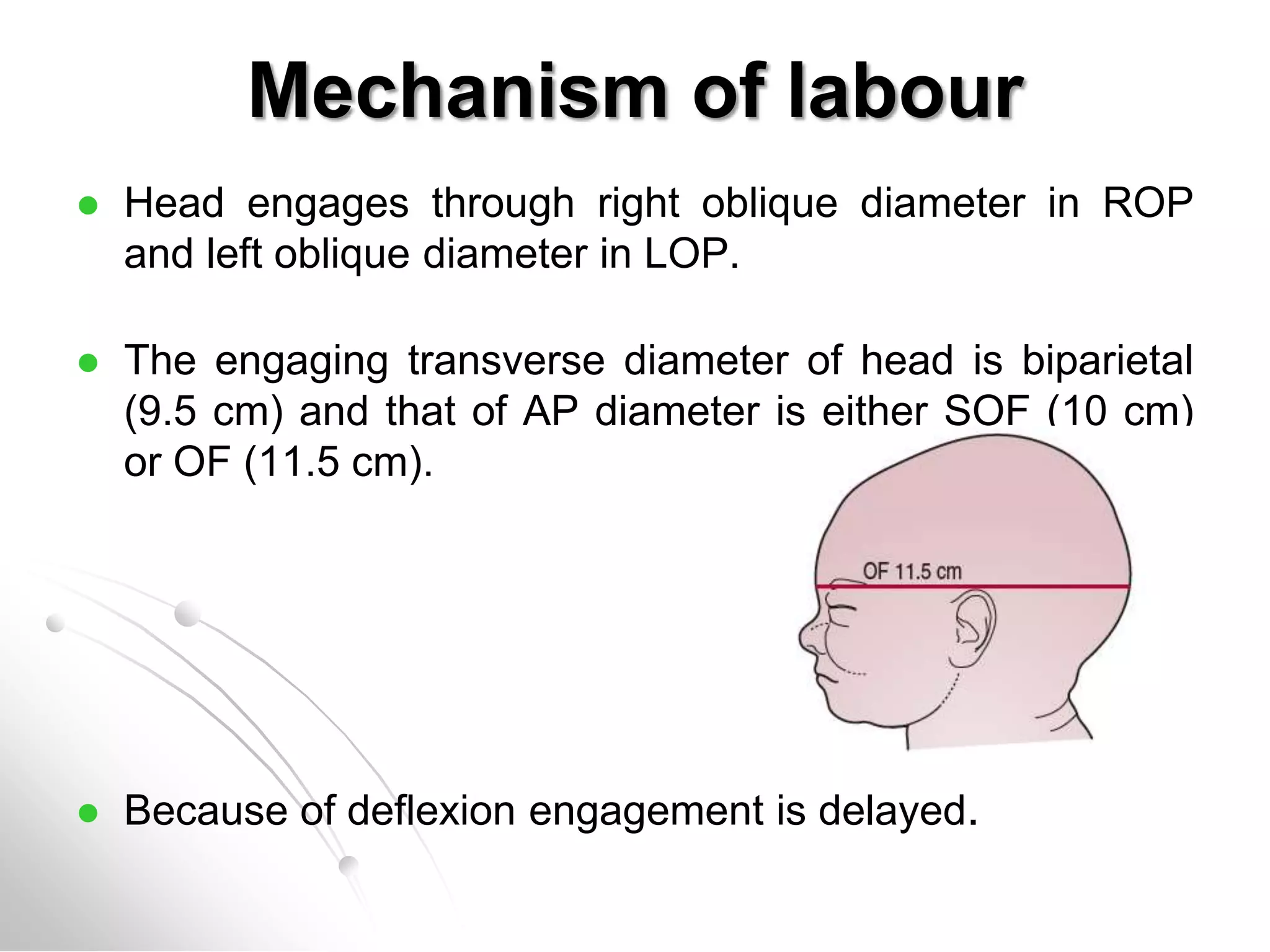
















This document provides information about occipito-posterior (OP) position during labor and delivery. It defines OP as the vertex position where the occiput is placed posteriorly. It discusses causes of OP position, abdominal and vaginal examination findings, the mechanism of labor including internal rotation and arrest issues. It also outlines diagnosis, management including care of the mother, complications, and references several textbooks on obstetrics.

















































































