Downloaded 3,694 times






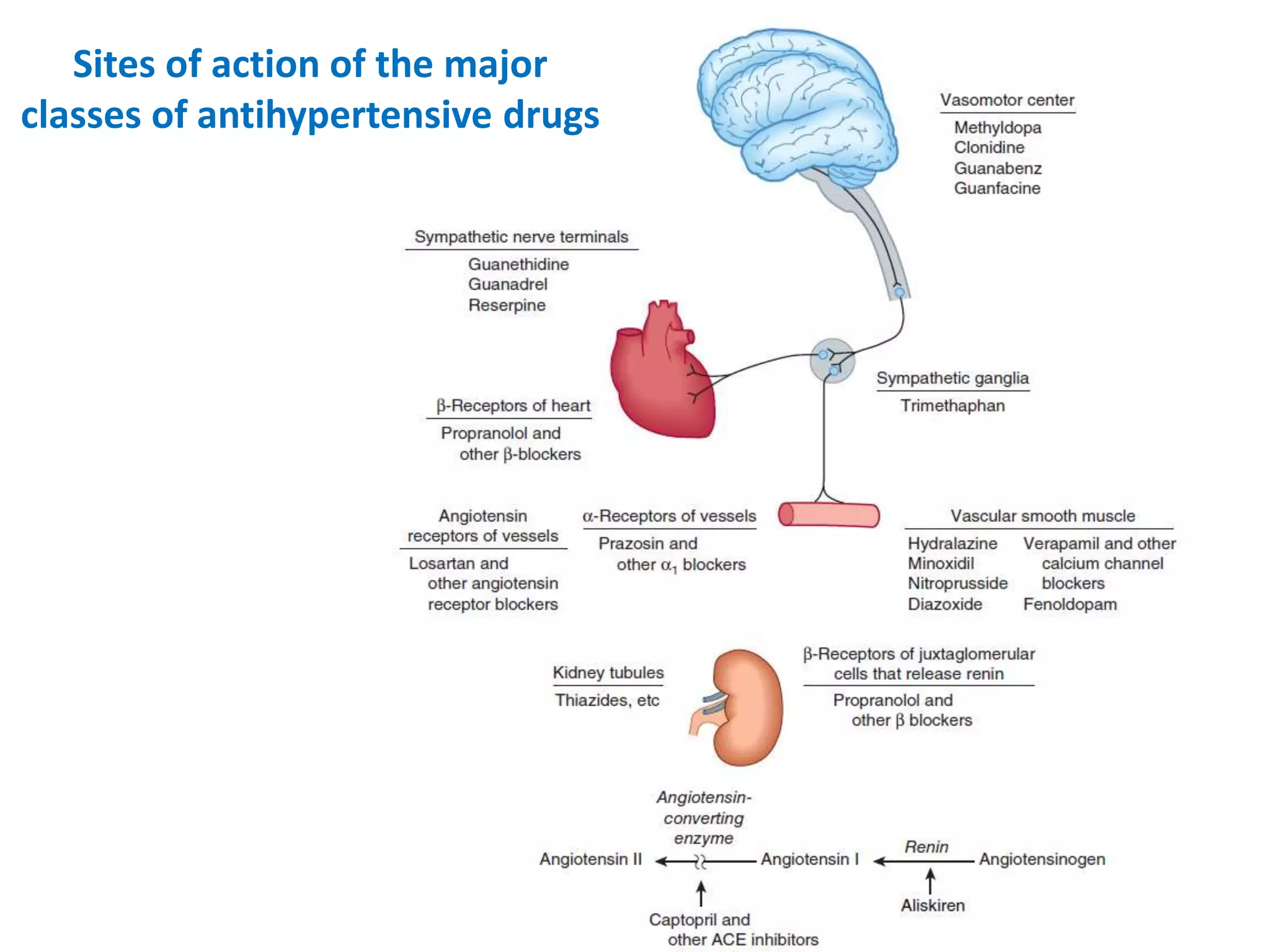





































1. The document discusses antihypertensive drugs, their mechanisms of action, and treatment of hypertension. It covers major classes of antihypertensive drugs including diuretics, ACE inhibitors, angiotensin receptor blockers, beta blockers, calcium channel blockers, and vasodilators. 2. It provides details on how each drug class lowers blood pressure by reducing peripheral vascular resistance, cardiac output, or sodium retention. Common side effects and advantages are also summarized for each drug class. 3. Guidelines for treating different stages of hypertension are presented, including recommendations to start with monotherapy or 2-drug combinations depending on severity, and to follow an A-B-C-D approach























































































