



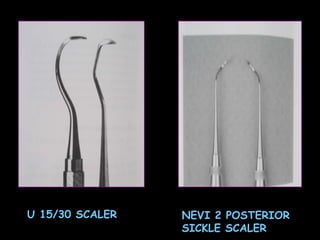
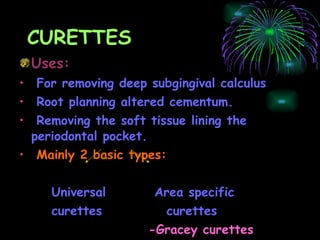









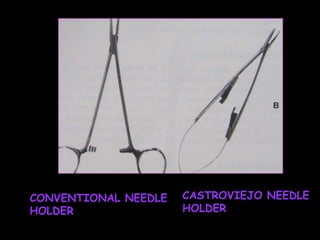




The document describes various periodontal instruments used for tasks like removing calculus, planning root surfaces, and curing gingiva. It classifies and discusses periodontal probes, explorers, scalers, curettes, ultrasonic/sonic instruments, the periodontal endoscope, and other instruments. It provides details on their design, parts, uses, and techniques for proper instrumentation.





































































































