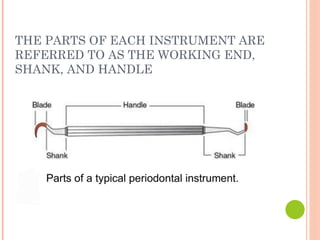
The document details the classification and functions of periodontal instruments used in dentistry, focusing on their specific purposes for scaling, curettage, and probing. It describes various types of instruments, including periodontal probes, explorers, scaling instruments, and ultrasonic devices, along with their designs and intended uses. Additionally, it covers advanced technologies such as digital probes and ultrasonic scalers, enhancing the diagnosis and treatment of periodontal disease.