Downloaded 112 times

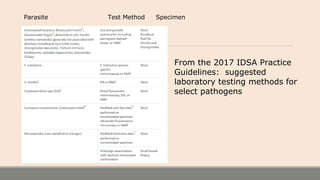
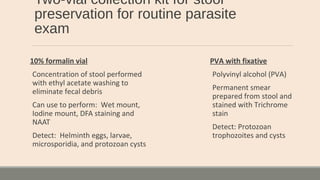
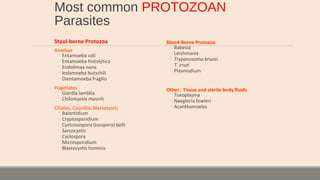
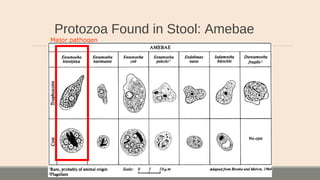
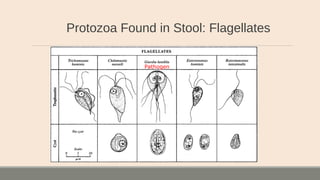
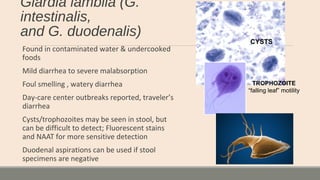
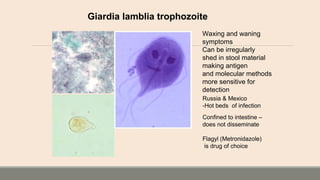

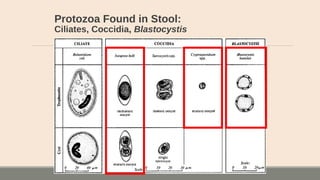
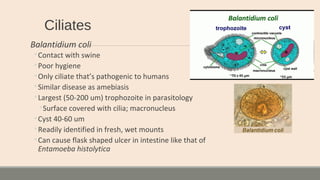
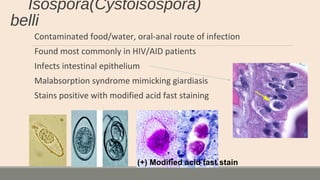
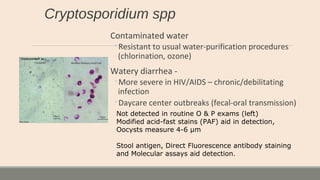
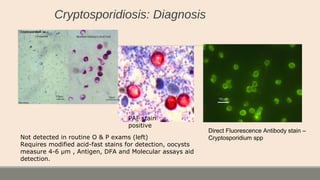






This document discusses parasitic infections that can cause diarrhea. It focuses on the laboratory diagnosis of parasitic infections through microscopic examination of stool and other specimens. The most common protozoan parasites found in stool are described in detail, including Entamoeba histolytica, Giardia lamblia, Cryptosporidium species, and others. Diagnostic methods for specific parasites are also outlined.













































![3-_Giardia_lamblia[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/3-giardialamblia1-230308222541-5f0a9947-thumbnail.jpg?width=640&height=640&fit=bounds)









































