Objectives
• Bacteriology isa massive area of study, and it is impossible to
review everything in this slide set.
• This lecture reviews the most important organisms and
laboratory tests, and relevant antimicrobial therapy
• There has been many taxonomic updates over the last few
years. There are guidelines for the reporting of taxonomic name
changes. The retired name is noted in parenthesis, such as
Kocuria (Micrococcus) kristinae.
3.
Safety in aBacteriology Laboratory
• Risk assessment should be performed for all activities to establish safety
precautions for a safe working environment.
• Bacteriology laboratories handling routine cultures are considered
Biosafety Level 2.
• Biosafety Level 2 (BSL-2) is appropriate for handling moderate-risk
agents that cause human disease of varying severity by ingestion or
through percutaneous or mucous membrane exposure.
• Clinical specimens and procedures with possible aerosolization or
splashing performed in Biosafety Level 2 Cabinets with HEPA filtration
• Gloves and impermeable lab coats when working with patient specimens
• Waste management program to properly dispose of biohazards
4.
Begin with Definitions
•Obligate Aerobe – require high level of oxygen (20%) to grow
• Microaerophilic – grow best with reduced oxygen and elevated % of
carbon dioxide
• Capnophilic – Requires high % carbon dioxide to grow
• Obligate Anaerobe – >30 min exposure to oxygen can be deadly
• Aerotolerant anaerobes– anaerobe is not killed by prolonged exposure to oxygen,
but grow best anaerobically, example: Clostridium tertium
• Facultative anaerobes – grow in both aerobic and anaerobic conditions
• Lag Phase - >24 hrs growth on agar plates, not appropriate for
biochemical or susceptibility testing
• Stationary phase – Organisms alive but not replicating, method for
transportation of patient specimens
5.
Specimen Collection –Aerobic and Facultative anaerobe
Throat / Wound / Abscess specimens
1. Swab collection using a Polyester fiber or flocked (prickly sponge)
2. Swab placed in Stuart’s or Amie’s transport media (buffer solution
with peptones)
3. Transport media preserves viability of the organisms, but does not promote
growth, provides stasis of numbers prior to plating onto solid agar, stability
limit <= 72 hours
4. *Cotton fiber swabs should not be used, traps bacteria and potentially toxic
Urine (2 commonly used methods)
1. Boric acid preservative, organisms in stationary phase for transport
2. Refrigerate urine at 4*C within one hour after collection
Both maintain original colony count and viability of organisms
for <= 24 hours
Tissues/Sterile body fluid
1. Adequate volume of fluid placed in sterile container.
6.
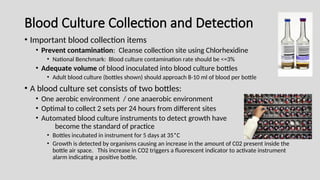
Blood Culture Collectionand Detection
• Important blood collection items
• Prevent contamination: Cleanse collection site using Chlorhexidine
• National Benchmark: Blood culture contamination rate should be <=3%
• Adequate volume of blood inoculated into blood culture bottles
• Adult blood culture (bottles shown) should approach 8-10 ml of blood per bottle
• A blood culture set consists of two bottles:
• One aerobic environment / one anaerobic environment
• Optimal to collect 2 sets per 24 hours from different sites
• Automated blood culture instruments to detect growth have
become the standard of practice
• Bottles incubated in instrument for 5 days at 35*C
• Growth is detected by organisms causing an increase in the amount of C02 present inside the
bottle air space. This increase in CO2 triggers a fluorescent indicator to activate instrument
alarm indicating a positive bottle.
7.
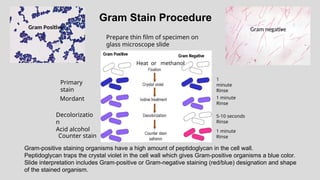
Gram Stain Procedure
1
minute
Rinse
Primary
stain
Mordant1 minute
Rinse
5-10 seconds
Rinse
Decolorizatio
n
Acid alcohol
Counter stain
1 minute
Rinse
Gram-positive staining organisms have a high amount of peptidoglycan in the cell wall.
Peptidoglycan traps the crystal violet in the cell wall which gives Gram-positive organisms a blue color.
Slide interpretation includes Gram-positive or Gram-negative staining (red/blue) designation and shape
of the stained organism.
Prepare thin film of specimen on
glass microscope slide
Heat or methanol
Gram Positive Gram negative
8.
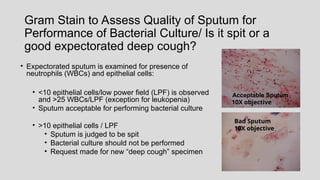
Gram Stain toAssess Quality of Sputum for
Performance of Bacterial Culture/ Is it spit or a
good expectorated deep cough?
• Expectorated sputum is examined for presence of
neutrophils (WBCs) and epithelial cells:
• <10 epithelial cells/low power field (LPF) is observed
and >25 WBCs/LPF (exception for leukopenia)
• Sputum acceptable for performing bacterial culture
• >10 epithelial cells / LPF
• Sputum is judged to be spit
• Bacterial culture should not be performed
• Request made for new “deep cough” specimen
Bad Sputum
10X objective
Acceptable Sputum
10X objective
9.
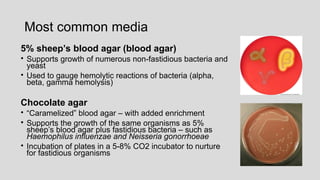
Most common media
5%sheep’s blood agar (blood agar)
• Supports growth of numerous non-fastidious bacteria and
yeast
• Used to gauge hemolytic reactions of bacteria (alpha,
beta, gamma hemolysis)
Chocolate agar
• “Caramelized” blood agar – with added enrichment
• Supports the growth of the same organisms as 5%
sheep’s blood agar plus fastidious bacteria – such as
Haemophilus influenzae and Neisseria gonorrhoeae
• Incubation of plates in a 5-8% CO2 incubator to nurture
for fastidious organisms
10.
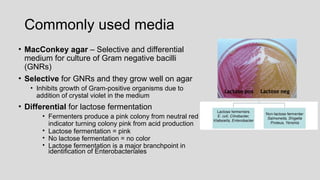
Commonly used media
•MacConkey agar – Selective and differential
medium for culture of Gram negative bacilli
(GNRs)
• Selective for GNRs and they grow well on agar
• Inhibits growth of Gram-positive organisms due to
addition of crystal violet in the medium
• Differential for lactose fermentation
• Fermenters produce a pink colony from neutral red
indicator turning colony pink from acid production
• Lactose fermentation = pink
• No lactose fermentation = no color
• Lactose fermentation is a major branchpoint in
identification of Enterobacteriales
Lactose pos Lactose neg
11.
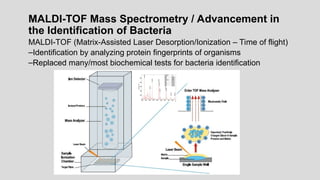
MALDI-TOF Mass Spectrometry/ Advancement in
the Identification of Bacteria
MALDI-TOF (Matrix-Assisted Laser Desorption/Ionization – Time of flight)
–Identification by analyzing protein fingerprints of organisms
–Replaced many/most biochemical tests for bacteria identification
12.
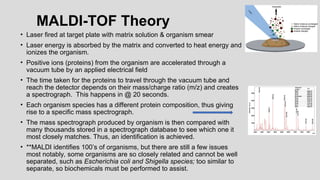
MALDI-TOF Theory
• Laserfired at target plate with matrix solution & organism smear
• Laser energy is absorbed by the matrix and converted to heat energy and
ionizes the organism.
• Positive ions (proteins) from the organism are accelerated through a
vacuum tube by an applied electrical field
• The time taken for the proteins to travel through the vacuum tube and
reach the detector depends on their mass/charge ratio (m/z) and creates
a spectrograph. This happens in @ 20 seconds.
• Each organism species has a different protein composition, thus giving
rise to a specific mass spectrograph.
• The mass spectrograph produced by organism is then compared with
many thousands stored in a spectrograph database to see which one it
most closely matches. Thus, an identification is achieved.
• **MALDI identifies 100’s of organisms, but there are still a few issues
most notably, some organisms are so closely related and cannot be well
separated, such as Escherichia coli and Shigella species; too similar to
separate, so biochemicals must be performed to assist.
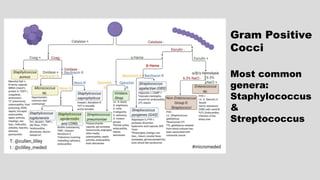
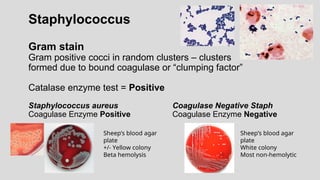
Staphylococcus
Gram stain
Gram positivecocci in random clusters – clusters
formed due to bound coagulase or “clumping factor”
Catalase enzyme test = Positive
Staphylococcus aureus Coagulase Negative Staph
Coagulase Enzyme Positive Coagulase Enzyme Negative
Sheep’s blood agar
plate
+/- Yellow colony
Beta hemolysis
Sheep’s blood agar
plate
White colony
Most non-hemolytic
15.
Catalase Enzyme Reaction
NegativePositive
Bacteria placed in Hydrogen
Peroxide/ bubbles = positive
reaction
Slide Coagulase reaction
Staphylococcus organism emulsified in rabbit plasma/
mix well. Positive = agglutination
Tube Coagulase Reaction
Rabbit plasma inoculated with organism and
incubated at 35˚C, observe for clot formation
at 4 hours. If no clot at 4 hours, observe at 24 hours
Negative tube coagulase
No clot formed/liquid =
Coagulase negative Staph
Positive Tube Coagulase
Clot formed at either 4 or
24 hours = Staph aureus
Slide Coagulase Reaction
Coagulase negative
Staphylococcus
Staph
aureus
16.
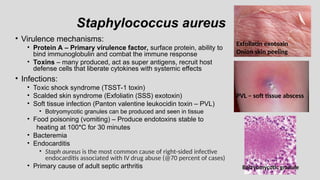
Staphylococcus aureus
• Virulencemechanisms:
• Protein A – Primary virulence factor, surface protein, ability to
bind immunoglobulin and combat the immune response
• Toxins – many produced, act as super antigens, recruit host
defense cells that liberate cytokines with systemic effects
• Infections:
• Toxic shock syndrome (TSST-1 toxin)
• Scalded skin syndrome (Exfoliatin (SSS) exotoxin)
• Soft tissue infection (Panton valentine leukocidin toxin – PVL)
• Botryomycotic granules can be produced and seen in tissue
• Food poisoning (vomiting) – Produce endotoxins stable to
heating at 100*C for 30 minutes
• Bacteremia
• Endocarditis
• Staph aureus is the most common cause of right-sided infective
endocarditis associated with IV drug abuse (@70 percent of cases)
• Primary cause of adult septic arthritis
Exfoliatin exotoxin
Onion skin peeling
PVL – soft tissue abscess
Botryomycotic granule
17.
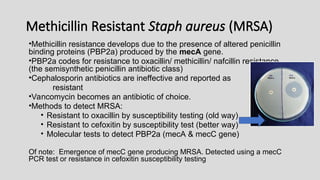
Methicillin Resistant Staphaureus (MRSA)
•Methicillin resistance develops due to the presence of altered penicillin
binding proteins (PBP2a) produced by the mecA gene.
•PBP2a codes for resistance to oxacillin/ methicillin/ nafcillin resistance
(the semisynthetic penicillin antibiotic class)
•Cephalosporin antibiotics are ineffective and reported as
resistant
•Vancomycin becomes an antibiotic of choice.
•Methods to detect MRSA:
• Resistant to oxacillin by susceptibility testing (old way)
• Resistant to cefoxitin by susceptibility test (better way)
• Molecular tests to detect PBP2a (mecA & mecC gene)
Of note: Emergence of mecC gene producing MRSA. Detected using a mecC
PCR test or resistance in cefoxitin susceptibility testing
18.
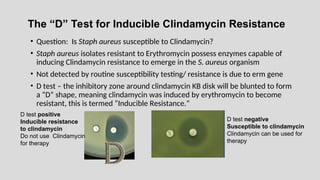
The “D” Testfor Inducible Clindamycin Resistance
• Question: Is Staph aureus susceptible to Clindamycin?
• Staph aureus isolates resistant to Erythromycin possess enzymes capable of
inducing Clindamycin resistance to emerge in the S. aureus organism
• Not detected by routine susceptibility testing/ resistance is due to erm gene
• D test – the inhibitory zone around clindamycin KB disk will be blunted to form
a “D” shape, meaning clindamycin was induced by erythromycin to become
resistant, this is termed “Inducible Resistance.”
D test positive
Inducible resistance
to clindamycin
Do not use Clindamycin
for therapy
D test negative
Susceptible to clindamycin
Clindamycin can be used for
therapy
19.
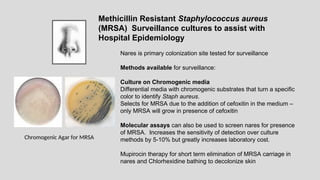
Nares is primarycolonization site tested for surveillance
Methods available for surveillance:
Culture on Chromogenic media
Differential media with chromogenic substrates that turn a specific
color to identify Staph aureus.
Selects for MRSA due to the addition of cefoxitin in the medium –
only MRSA will grow in presence of cefoxitin
Molecular assays can also be used to screen nares for presence
of MRSA. Increases the sensitivity of detection over culture
methods by 5-10% but greatly increases laboratory cost.
Mupirocin therapy for short term elimination of MRSA carriage in
nares and Chlorhexidine bathing to decolonize skin
Methicillin Resistant Staphylococcus aureus
(MRSA) Surveillance cultures to assist with
Hospital Epidemiology
Chromogenic Agar for MRSA
20.
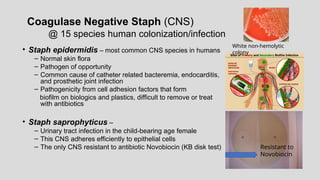
Coagulase Negative Staph(CNS)
@ 15 species human colonization/infection
• Staph epidermidis – most common CNS species in humans
– Normal skin flora
– Pathogen of opportunity
– Common cause of catheter related bacteremia, endocarditis,
and prosthetic joint infection
– Pathogenicity from cell adhesion factors that form
biofilm on biologics and plastics, difficult to remove or treat
with antibiotics
• Staph saprophyticus –
– Urinary tract infection in the child-bearing age female
– This CNS adheres efficiently to epithelial cells
– The only CNS resistant to antibiotic Novobiocin (KB disk test)
White non-hemolytic
colony
Resistant to
Novobiocin
21.
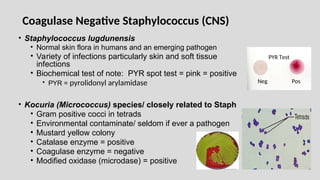
• Staphylococcus lugdunensis
•Normal skin flora in humans and an emerging pathogen
• Variety of infections particularly skin and soft tissue
infections
• Biochemical test of note: PYR spot test = pink = positive
• PYR = pyrolidonyl arylamidase
• Kocuria (Micrococcus) species/ closely related to Staph
• Gram positive cocci in tetrads
• Environmental contaminate/ seldom if ever a pathogen
• Mustard yellow colony
• Catalase enzyme = positive
• Coagulase enzyme = negative
• Modified oxidase (microdase) = positive
Neg Pos
PYR Test
Coagulase Negative Staphylococcus (CNS)
22.
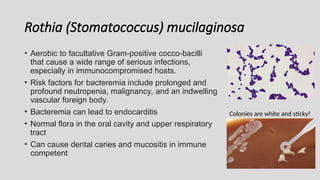
Rothia (Stomatococcus) mucilaginosa
•Aerobic to facultative Gram-positive cocco-bacilli
that cause a wide range of serious infections,
especially in immunocompromised hosts.
• Risk factors for bacteremia include prolonged and
profound neutropenia, malignancy, and an indwelling
vascular foreign body.
• Bacteremia can lead to endocarditis
• Normal flora in the oral cavity and upper respiratory
tract
• Can cause dental caries and mucositis in immune
competent
Colonies are white and sticky!
23.
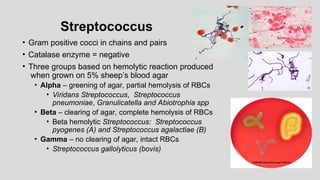
Streptococcus
• Gram positivecocci in chains and pairs
• Catalase enzyme = negative
• Three groups based on hemolytic reaction produced
when grown on 5% sheep’s blood agar
• Alpha – greening of agar, partial hemolysis of RBCs
• Viridans Streptococcus, Streptococcus
pneumoniae, Granulicatella and Abiotrophia spp
• Beta – clearing of agar, complete hemolysis of RBCs
• Beta hemolytic Streptococcus: Streptococcus
pyogenes (A) and Streptococcus agalactiae (B)
• Gamma – no clearing of agar, intact RBCs
• Streptococcus gallolyticus (bovis)
24.
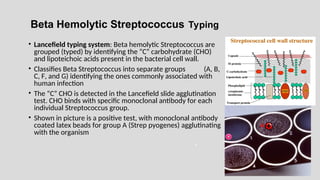
Beta Hemolytic StreptococcusTyping
• Lancefield typing system: Beta hemolytic Streptococcus are
grouped (typed) by identifying the “C” carbohydrate (CHO)
and lipoteichoic acids present in the bacterial cell wall.
• Classifies Beta Streptococcus into separate groups (A, B,
C, F, and G) identifying the ones commonly associated with
human infection
• The “C” CHO is detected in the Lancefield slide agglutination
test. CHO binds with specific monoclonal antibody for each
individual Streptococcus group.
• Shown in picture is a positive test, with monoclonal antibody
coated latex beads for group A (Strep pyogenes) agglutinating
with the organism
-
A
25.
Streptococcus pyogenes
• GroupA Streptococcus [GAS] – of 5% Sheep’s blood agar produces
an intense ring of beta hemolysis around a small grey colony
• Biochemical tests used for identification:
• Bacitracin KB sensitivity test – GAS is inhibited by antibiotic
Bacitracin (A) producing a small zone of inhibition
• Not specific for GAS, inhibition also occurs with Beta hemolytic
Streptococcus group C, test is seldom used
• PYR (pyrrolidonyl arylmidase) reaction
• Organism spotted onto moist PYR disk
• Wait 2 min – room temperature incubation
• Add cinnamaldehyde reagent
• Pink = positive = Streptococcus pyogenes
• **This test is not exclusive for Strep pyogenes –
Enterococcus and Staph lugdunensis also test positive
• Therapy : Penicillin, Amoxicillin or Cephalosporin antibiotics
No resistance reported to these agents
PYR reaction
+ --
26.
• Streptolysin Oand Streptolysin S toxins
• Comprise the ASO titer assay used to diagnose Strep
pyogenes sequelae (rheumatic fever and
glomerulonephritis)
• These toxins help GAS evade the immune system
• Toxin activity can be visually demonstrated on 5% Sheep’s
blood agar
• Streptolysin O toxin is oxygen labile
• Streptolysin S toxin is oxygen stable
• When both toxins are present, the stabbed area of the
media will demonstrate increased beta hemolysis
Strep pyogenes (GAS) virulence factors
•M Protein prevents phagocytosis
•Hyaluronic capsule prevents phagocytosis
Sequelae of Streppyogenes Infection
Rheumatic fever
• Inadequate treatment of GAS skin infection or pharyngitis
• Family history, strain of GAS and multiple exposures can more
likely evolve into sequelae, occurs 10-30 days post infection
• Usually occurs in children 5 – 15 years
• Pathogenicity due to molecular mimicry: similarity between the proteins of
Strep A and human muscle tissue causes an autoimmune mechanism
that leads to confusion. The immune system is then armed to attack heart
(heart valves, muscle), joint, and bones not just GAS
• Usually leads to need for valve replacement surgery
Glomerulonephritis
• Post infection with Nephritogenic strain of GAS
• Leads to immune mediated destruction of renal glomeruli
• Usually resolves without therapy but can progress
29.
Streptococcus agalactiae (GBS)
•Biochemical tests:
– Camp test – Staph aureus strain that contains Camp factor streaked
perpendicular to group B Strep on a 5% sheep’s blood agar plate, Incubate 24 hr.
and view for intensified arrow shaped hemolysis. Positive test = GBS (see pix)
– Hippurate hydrolysis – used to detect the ability of GBS to hydrolyze the
chemical Hippurate, into glycine and benzoic acid by action of the
hippuricase enzyme. Positive test = purple
pos
Staph aureus
Strep group B
Camp Test
Hippurate Hydrolysis
Increased area of
hemolysis
30.
Streptococcus agalactiae (GBS)
•Pathogen of elderly
• Bacteremia and urinary tract infection,
• Acquisition most likely from the intestine
• Pathogen of neonate
• Bacteremia or central nervous system infection
• In utero or perinatal organism acquisition during birthing process,
• Infection in @ 1/2000 births
• Early onset infection within 7 days of birth
• Late onset infection 8 – 28 days after birth
• Treatment: Penicillin or Cephalosporin (3rd
generation)
31.
Streptococcus agalactiae (GBS)
•Most effective way to prevent GBS neonatal infection is detect
colonization in pregnant
• Pregnant colonized (>=25%) in the cervix and/or rectal area
• All pregnant should be screened at 35 – 37 weeks of pregnancy
(Regulation/standard of practice)
• Enrichment method for GBS screening mandatory
• Cervix and rectal swab incubated in an enrichment broth (LIM or
carrot broth) for 18 hours at 35 ˚C then cultured onto 5% sheep’s
blood agar.
• Initial incubation in Enrichment broth is used to increase
sensitivity in molecular detection assays.
• Ampicillin drug of choice for prophylaxis of pregnant women
testing positive for GBS.
• Susceptibility testing for alternative therapies must be performed in the
penicillin allergic patient (Clindamycin primary 2nd
line)
32.
Streptococcus pneumoniae
• Grampositive bullet (lancet) shaped cocci in pairs
• Polysaccharide capsule = virulence factor / antiphagocytic
• Alpha hemolytic on 5% Sheep’s blood agar
• Mucoid due to large amount of capsule production
• Identification:
• Bile soluble – colonies dissolve Inhibited by Optochin –
in sodium deoxycholate (bile) ethylhydrocupreine
hydrochloride
Zone of inhibition
must be >=14 mm
Autolytic Changes
Looks like tire
33.
Streptococcus pneumoniae
• Normalinhabitant of the upper respiratory tract
• Infections: Upper and Lower respiratory tract infection (Lobar
pneumonia), sepsis, meningitis, middle ear, ocular, sinus
• Asplenic and immune suppressed patients particularly at risk
• 13-20 valent pneumococcal conjugate vaccine aids in preventing
invasive infections – those at risk needing vaccination include infants,
HIV, immune suppressed, and elderly
• Susceptibility issues:
• Acquired resistance to Penicillin due to Penicillin binding proteins
can occur in @ 5% of isolates
• If susceptible,1st
line therapy usually 3rd
generation Cephalosporin
(Ceftriaxone)
34.
Viridans Streptococcus
• Severalspecies of viridans group Streptococcus are NF in mouth
and upper respiratory tract. Most common species:
S. mutans S. salivarius S. sanguis S. mitis
• Bile esculin negative
• Bile solubility negative
• Optochin resistant (zone size <=13 mm)
• Cause 30 – 40% cases of sub acute endocarditis on native valve,
usually due to bad dentition
• Cause abscess and various infections throughout the body in the
immune suppressed host
• Variable susceptibility patterns can have elevated MICs to
Penicillin so usual therapy is 3rd
generation cephalosporin.
Streptococcus
pneumoniae
Viridans
Streptococcus
35.
Viridans Streptococcus
unique species
•Streptococcus anginosis group:
• S. anginosus S. constellatus S. intermedius
• Normal flora in human mouth
• More virulent than “routine” viridans Streptococcus, due to capsule
• Grow best when incubated in 5 – 10% CO² incubation (microaerophilic)
• Butterscotch odor to colony
• Cause deep tissue abscess, bacteremia, endocarditis, and intra abdominal
infection
• Variable susceptibilities – susceptibility testing guides therapy, always
susceptible to vancomycin
36.
Nutritionally Variant Streptococcus
•Vitamin B6 (pyridoxal) deficient –
• Will not grow on agar medium without B6 supplementation
• Chocolate agar with supplements will support growth
• Will grow in blood culture bottle due to patient’s blood
containing vitamin B6
• Will not grow on 5% Sheep’s blood agar plate
• Will grow around Staph aureus streak for it supplies vitamin B6
• MALDI-TOF can definitively identify
• Two genera:
• Abiotrophia defectiva
• Granulicatella adiacens
• Bacteremia and Endocarditis –
• More destructive to valve than viridans Streptococcus species
• Elevated MIC’s to Penicillin, susceptible to 3rd
generation
Cephalosporins.
Satellite
next to S. aureus streak
37.
Streptococcus gallolyticus (bovis)
•Streptococcus gallolyticus ssp. gallolyticus (S. bovis biotype 1)
Isolation from blood culture is associated with colon cancer (73%)
• Streptococcus gallolyticus ssp. pasteurianus (S. bovis biotype 2)
Isolation from CSF in neonatal meningitis
• Gray colony, gamma hemolytic, Gram positive cocci in pairs and short chains
• Biochemical reactions:
Bile esculin slant = positive
6.5% NaCl = no growth
PYR reaction = negative
Susceptible to Penicillin
Bile Esculin Positive
6.5% No Growth 6.5% Growth
PYR Negative PYR Positive
Strep gallolyticus Enterococcus
38.
• Most commonspecies
• E. faecium and E. faecalis
• No defined virulence factors
• Gray colony, gamma hemolytic on 5% Sheep’s blood agar
• Gram positive cocci in pairs and short chains
• Biochemical tests:
• Bile esculin agar pos = grows in presence of bile &
reduces esculin to esculetin to produce black color
• 6.5% NaCl tolerance = grows in presence of NaCl
• PYR reaction = positive
• E. faecium = arabinose fermentation positive
• E. faecalis = arabinose fermentation negative
Enterococcus
+ -
PYR
Neg Pos
39.
Enterococcus
• Pathogen ofopportunity
• Normal human intestinal flora
• Infections include UTI, bacteremia, and abdominal abscess
• Antimicrobial therapy:
• Intrinsic resistance to cephalosporin antibiotics
• Ampicillin plus Aminoglycoside can be synergistic for therapy of
endocarditis
• Vancomycin is an antibiotic of choice
• Unique susceptibility issue
• Acquired resistance to vancomycin known as vancomycin resistant
enterococcus or VRE. Resistance is due to acquisition of genetic
resistance genes:
• Van A resistance gene for E. faecium
• Van B resistance gene for E. faecalis
40.
Opportunistic Gram positivecocci
• Aerococcus ureae – Gram positive cocci in pairs and clusters
• Alpha hemolytic on 5% Sheep’s blood agar , difficult to identify with
biochemicals, often confused with viridans Streptococcus, MALDI-TOF ID
• Emerging urinary tract pathogen
• Gemella morbillorum– Gram positive cocci in pairs
• Microaerophilic
• Normal flora in oral cavity
• Bacteremia with endocarditis
• Leuconostoc mesenteroides– Gram positive cocci in chains
• Intrinsic resistance to vancomycin
• Bile esculin = negative
• Bacteremia in immune suppressed
• Watch out! Do not confuse with vancomycin resistant enterococcus (VRE)
Gram Negative Cocci
•Neisseria species and Moraxella catarrhalis
• Small kidney bean shaped cocci in pairs
• Oxidase enzyme = positive
• CTA (Cysteine Trypticase Agar) carbohydrate fermentation
tests, older method to biochemically identify
• N. gonorrhoeae Gluc + Mal - Lac - Suc -
• N. meningitidis Gluc + Mal + Lac - Suc -
• N. lactamica Gluc + Mal + Lac+ Suc-
• M. catarrhalis Gluc - Mal - Lac - Suc -
• N. gonorrhoeae will NOT grow on 5% Sheep’s blood agar
• N. meningitidis grows on 5% Sheep’s blood agar
+ +
43.
Carbohydrate Fermentation Reactionsfor Neisseria
Compare (+) yellow fermentation
reaction to negative (red) control
well
+
Oxidase enzyme spot test:
•Detects production of enzyme
cytochrome oxidase
•Add reagent N,N trimethyl-p-
phenylenediamine dihydrochloride to
filter paper with organism smear
•Positive = blue to purple color
Control
neg
Growth on Chocolate Agar
Oxidase Enzyme Positive
Glucose + Glucose+/Maltose +
N. gonorrhoeae N. meningitidis
No growth BAP Grows on BAP
Negative
Positive
44.
Neisseria meningitidis
• Colonizationoccurs in nasopharynx (10-20%)
• African meningitis belt – highest prevalence of disease in world
• Meningitis, usually occurring in children and young adults
• Hallmark - petechiae (organisms crowd into capillaries) leads to
tissue necrosis and disseminated intravascular coagulation (DIC)
from endotoxin production
• Progressive infection can be rapidly fatal (<24hrs)
• Primary virulence factor is capsular polysaccharide
• N. meningitidis 13 serotypes A,B,C Y and W, most common
• Serotypes C, Y, and B are ones most common in the US
• Complement deficiencies in factors 7, 8, and 9, Eculizumab therapy,
asplenia, and HIV predispose to infection
• Adrenal necrosis known as Waterhouse Friderichsen syndrome
• Preventative Immunization at ages 2m, 12 yr, 16 yr, and in HIV
Petechiae
45.
Neisseria gonorrhoeae
• Sexuallytransmitted infection: most common sites of infection include
urethrae, endocervix, ocular, rectal, oropharynx, monoarticular arthritis
• 10-20 % female ascend to PID but only 0.5% disseminate into bloodstream
• Gram stain of urethral discharge useful for male diagnosis
• Gram stain of cervix problematic due to NF look-a-like organisms
• Specimen collection culture :charcoal swabs, do not refrigerate
• Media: Selective Thayer Martin or Martin Lewis agars
• Chocolate agars with increased nutritional supplementation and antibiotics
trimethoprim, vancomycin, polymyxin, and nystatin
• Resistance: Beta lactamase enzyme and Chromosomal resistance
• Emerging resistance in SE Asia has increased the necessity to perform
susceptibility assessment for patients not responding to first line therapies
• Therapy: 1st line Ceftriaxone + Azithromycin or Doxycycline
46.
Molecular testing for
Moleculartesting for Neisseria gonorrhoeae
Neisseria gonorrhoeae
• Standard of practice and mostly combo testing with
Standard of practice and mostly combo testing with Chlamydia trachomatis
Chlamydia trachomatis
due to high % of co-infections
due to high % of co-infections
• Urine, cervix/vaginal, throat, and rectal are sites most often tested
Urine, cervix/vaginal, throat, and rectal are sites most often tested
• Molecular testing sensitive (96%) and specific (99%)
Molecular testing sensitive (96%) and specific (99%)
• Female: best specimen for diagnosis is cervix
Female: best specimen for diagnosis is cervix
• Urine <=10–15% less sensitive than cervix specimen
Urine <=10–15% less sensitive than cervix specimen
• Male: Urine is the standard specimen for diagnostic testing
Male: Urine is the standard specimen for diagnostic testing
• The older way for diagnosing
The older way for diagnosing Chlamydia trachomatis
Chlamydia trachomatis infection
infection:
:
C. trachomatis cell culture -
Iodine staining of inclusions
in McCoy cell line culture
Fluorescent antibody staining of
C. trachomatis infected cell –
green staining Elementary
bodies indicates infected cell.
47.
Moraxella catarrhalis
• Colonizesthe upper respiratory tract
• Infections: Pneumonia (COPD), sinusitis, primary cause of otitis
media in young children
• Sputum Gram stain can be helpful in diagnosis of pneumonia
• Hockey puck colony – able to push colony across the agar
surface without disruption
• Biochemical Tests:
• Oxidase enzyme positive
• DNA’ase enzyme positive
• Indoxyl butyrate positive
• Antimicrobial resistance: beta lactamase enzyme production
(90%) eliminating Ampicillin for therapy
• Therapy: Augmentin or 3rd
generation Cephalosporin
Sputum = PMS’s and Gram
negative diplococci
Corynebacterium
•Over 20 species,most are saprophytic
• Human normal flora, skin and nares
•Most grow well on 5% Sheep’s blood agar
•Gamma hemolytic gray colonies , no hemolysis
•Catalase enzyme = positive
•“Diphtheroid” morphology on staining, ie. Gram
positive rods in Chinese letter forms
•No spores produced
50.
Corynebacterium diphtheriae
• Diphtheria
•Forms tough oropharyngeal membrane (Diphtheroid Greek for leather),
bleeds when attempt to remove
• Phage mediated exotoxin is distributed from the membrane causing
respiratory paralysis, heart, nervous system, and kidney damage
• Non-toxin producing strains can cause cutaneous lesions and
ulcers; crowded or unsanitary conditions
• Diagnosis: culture with toxin detection at public health
department (usually by Elek plate), serology, and/or PCR to
detect organism and detect toxin genes
• Grows well on 5% Sheep’s blood agar, producing gray gamma
hemolytic colonies
• Selective media: Cysteine Tellurite and Tinsdale agar - black
colonies produced on both media.
• Treatment: Anti-toxin plus Erythromycin or Penicillin
Line of precipitation formed
with toxin from organism reacting
with antitoxin on paper strip.
Elek Plate
51.
Other Corynebacterium spp.
•C. jeikeium
• Normal human skin flora / thrives on lipid
• Infects patients by invading indwelling plastic catheters
• Biofilms are formed on the plastic which protects the organisms from
being killed by antibiotic treatment
• Susceptible to vancomycin and tetracycline
• C. urealyticum
• Urease enzyme positive
• Cause of urinary tract infection in post renal transplants
• Resistant to many antibiotics but vancomycin susceptible
• C. macginleyi
• Conjunctivitis, keratitis (contact lens wearers) and endophthalmitis
• C. kroppenstedtii
• NF on the skin and can cause granulomatous globular mastitis
Red is (+) for
Urease reaction
+
Biofilm
52.
•Rhodoccocus equi
• Relatedto Nocardia and Mycobacterium species
• Partially acid fast (PAF) with modified acid-fast staining
• Unique salmon pink colored colony
• Environmental, found in soil, and zoonotic pathogen
• Can cause human pneumonia, bacteremia with tissue invasion
and is most common in immune suppressed, HIV
•Arcanobacterium haemolyticum
• Cause of pharyngitis in children
• Beta hemolytic colonies and catalase negative can lead to
possible confusion with Streptococcus pyogenes
• Maldi-TOF supplies identification
• Reverse CAMP test positive
Salmon pink colonies at 35*C
Gram positive coccobacilli
53.
Bacillus species
• LargeGram positive rods – box car shaped with square ends
• Gram stain: Can be easily over-decolorized may appear red in color
Spores will not stain causing a clear area in the organism
• Catalase enzyme positive
Spores/ clear areas
in bacillus
Variable staining / not
clearly Gram positive Spore stain
54.
Bacillus anthracis
• CategoryA agent – Biothreat pathogen
• Any suspicion of infected patient, notify local public health department
• Agent of anthrax in herbivores
• Virulence factors: anthrax toxin and capsular polypeptide
• Infections:
• Wool sorter’s disease – usually acquired from handling
contaminated cow hides, produces a unique black eschar skin lesion
• Systemic infections from breathing in spores or eating and drinking
infected food products. Pneumonia, sepsis, and meningitis
• Fatality rate >=50%
• Colony on 5% Sheep’s blood agar has an irregular colony border
Medusa head colonies (sticky consistency)
Whitish colony, Gamma hemolytic (no hemolysis)
Non-motile
Susceptible to penicillin
Wool sorter’s diseae
Medusa head colony
55.
Bacillus cereus
•Most commonBacillus species causing infection
•Saprophytic environmental organism
•Nosocomial and opportunistic infections, particularly in immunocompromised,
and patients with indwelling or implanted devices due to biofilm formation
• Can be either a contaminate or pathogen in positive blood cultures
• Can cause skin infections in intravenous drug users
•Food poisoning: vomiting due to emetic toxin production and diarrhea from
diarrheal toxin. Refried rice has always been prime food suspect.
•Gram positive rod with spore production
• Dull gray colony producing beta hemolysis on BAP
• Catalase positive
• Motile
• Resistant to penicillin
56.
Listeria monocytogenes
• Soil,water, sewage and animals (associated food)
• Small Gram positive rod / no spores produced
• Catalase enzyme positive
• Grows well on 5% sheep’s BAP producing subtle beta hemolysis
• Motility provides identifying information
• More motile at 25˚C than 35˚C
• Tumbling motility on wet mount examination
• Umbrella motility when inoculated into tubed media
• Bacteremia and meningitis in immune suppressed, pregnant,
neonates, and elderly
• Culture and/or molecular amplification methods for diagnosis
• Grows well at 4˚C, leading to food sources contaminated non
pasteurized cheese and milk products and Deli case foods
• Ampicillin drug of choice
• Intrinsic resistance to Cephalosporin antibiotics
Umbrella Motility
57.
Erysipelothrix
rhusiopathiae
• Small pleomorphicGram positive rod
• No spores produced
• Catalase enzyme negative
• Alpha hemolytic colony produced on 5% sheep’s blood agar
plate
• Only Gram positive rod that produces hydrogen sulfide (H2S)
• MALDI-TOF is helpful for this difficult to identify bacteria
• Infections acquired from nature and animals (swine), an occupational
disease of farmers and butchers known as Erysipeloid
• Virulence factor: capsule
• Soft tissue infection and bacteremia +/- endocarditis
• Intrinsic resistance to Vancomycin
H2S production detected
on
Triple sugar iron agar (TSI)
Swine Erysipelas – lacy
skin lesions of swine
Erysipeloid
59.
Enterobacteriales
Lactose Fermenters (PINKon
MacConkey agar) A
Non-lactose Fermenter (no
Color / MacConkey agar) B
Escherichia coli Proteus
Klebsiella Serratia
Enterobacter Salmonella
Citrobacter Shigella
Yersinia / Vibrio
60.
Triple Sugar IronAgar (TSI)– used to detect fermentation of glucose,
lactose and/or sucrose and production of hydrogen sulfide [H2S] in Gram negative
bacilli
CHO
Fermentation=
Yellow medium
Gas production=
Disruption of the
agar
No CHO
fermentation =
Red medium
H2S production
= black medium
at bottom of
tube
Pseudomonas Shigella E. coli Citrobacter Salmonella
61.
Enterobacterales
Escherichia coli
• Normalflora in human intestine
• #1 cause of urinary tract infections
• Also, bacteremia, neonatal meningitis, and
abdominal infections
• Lactose fermenter
• Eosin methylene blue agar (EMB) green sheen
produced
• Positive spot indole reaction / turns robin’s egg blue
• Organism grown on 5% Sheep’s blood agar plate is
smeared on filter paper spotted with one drop of indole
reagent
• Test must be performed from growth on Blood agar plate,
for blood agar contains tryptophan
• Indole is the breakdown product of tryptophan
Green sheen
EMB agar
Spot Indole:
Negative Positive
Lactose
Fermenter
MacConkey agar
62.
Escherichia coli
• Pathogen(s)of diarrhea: Molecular testing is standard of practice
• Enterotoxigenic (ETEC) E.coli cause of traveler’s diarrhea
• Enterohemorrhagic E.coli (EHEC, such as 0157:H7)
• Bloody diarrhea from eating undercooked beef or contaminated vegetables
from bad farm practices
• Pathogenicity from Shiga toxin production (STX-1 and STX-2)
• Progressive infection can lead to Hemolytic uremic syndrome (HUS) with
hemolytic anemia, thrombocytopenia, and renal failure, particularly occurring
in young children
• Old school: Culture stool on sorbitol containing MacConkey agar / EHEC
does NOT ferment sorbitol/ most all E. coli except EHEC ferment sorbitol.
Presumptive test.
• Less common with questionable significance, no therapy is needed
• Enteropathogenic (EPEC) E.coli rare cause of diarrhea in children
• Enteroinvasive (EIEC) E.coli rare cause of traveler’s diarrhea
63.
Enterobacter cloacae complex
•Environmentalsource, with low pathogenicity
•Usually infects only a compromised host
•Cronobacter (Enterobacter) sakazakii associated with neonatal
meningitis
Klebsiella species
•K. pneumoniae most common species
•Mucoid colony due to capsule production
•Currant jelly sputum produced in alcoholics due to blood mixed with
Klebsiella capsular polysaccharide
•Klebsiella (Enterobacter) aerogenes taxonomic re-classification
64.
Extended Beta LactamaseProduction
Extended Beta Lactamase Production
•Enzymes produced by select species of Enterobacterales
Enzymes produced by select species of Enterobacterales
• Confer resistance to Cephalosporins, Penicillins and
Confer resistance to Cephalosporins, Penicillins and
Monobactam (Aztreonam) antibiotics by opening the
Monobactam (Aztreonam) antibiotics by opening the
beta lactam ring of the antibiotic and inactivating the
beta lactam ring of the antibiotic and inactivating the
antibiotic
antibiotic
• ESBLs do not attack Cephamycin antibiotics (cefoxitin,
ESBLs do not attack Cephamycin antibiotics (cefoxitin,
cefotetan) or the Carbapenem antibiotic classes
cefotetan) or the Carbapenem antibiotic classes
• Enzymes are transported on plasmids
Enzymes are transported on plasmids
•Plasmid mediated CTX-M beta lactamase (bla gene) is the
Plasmid mediated CTX-M beta lactamase (bla gene) is the
most common ESBL enzyme in the US currently, but
most common ESBL enzyme in the US currently, but
many ESBL types can be found worldwide
many ESBL types can be found worldwide
•Therapy for ESBL producing Enterobacterales:
Therapy for ESBL producing Enterobacterales:
• Carbapenems: Imipenem, Meropenem, Doripenem, &
Carbapenems: Imipenem, Meropenem, Doripenem, &
Ertapenem
Ertapenem
65.
Carbapenemases – CREand CRO
•CRE = Carbapenemase resistant Enterobacteriales
CRO= Carbapenemase resistant organism (Pseudomonas)
•Carbapenemase beta lactamases lead to resistance to carbapenam
antibiotics (meropenem, imipenem, doripenem, ertapenem).
•Carbapenem-hydrolyzing-beta-lactamases are incorporated into the genetic
elements in transposons of Gram negative bacillus. Transposons can
insert into diverse plasmids which can transfer resistance to a broad
spectrum of Gram negative bacillus.
•Two CREs are getting the most attention:
• KPC – “Klebsiella pneumoniae carbapenemase” most common in the US
• NDM-1 – New Delhi metallo-beta-lactamase
• Other CRE/CROs: IMP, OXA-48, and VIM ….. Many others less common
•Infections with CRE/CRO producing GNRs can have a 50% fatality rate
66.
Gram Negative Rodsthat
do NOT Ferment Lactose!
• Proteus species
Colonies swarm in concentric layers on agar surface
• Proteus vulgaris – spot indole positive
• Proteus mirabilis – spot indole negative
• Normal flora in intestine
• Common cause of UTI and abdominal infections
• Intrinsic resistance to antibiotic Colistin due to mcr-1 gene
• Serratia marcescens
• Produces red pigmentation which can intensify at room temp
• Environmental contaminate
• Causes infection most usually in
• Immune suppressed
• Ventilator associated pneumonia
• Bacteremia
67.
• Salmonella species
•Diarrhea with +/- fever and PMNs in the stool
• Infection from eating contaminated food (raw eggs, poultry, ground
beef or dairy) or direct contact with a sick person or animal
– Must ingest large #’s of organisms to make you ill, normal levels
of stomach acid is protective
• MacConkey agar - does not ferment lactose
• Produces hydrogen sulfide on selective media
• Motile
• Identification based on biochemical reactions and serologic typing
• Kaufman White serologic typing for speciation of Salmonella
• O Somatic (cell wall) antigen – Salmonella group “B”
• H flagellar antigens – 2 phases [h1 & h2]
• Vi capsular antigen – Salmonella typhi only
68.
Salmonella typhi
• Typhoidfever – high fever and sepsis, not a diarrheal pathogen
• Human pathogen with most cases in US from international travel (75%)
• Post typhoid fever can result in carriage in gallbladder with passage in
feces. Can transmit to others with bad hygiene and food preparation
• Ingested organisms enter the bowel, rapidly move into the blood
stream and eventually the bone marrow
• Diagnosis: Blood cultures in early infection and bone marrow culture
in late stages (>1 month) of infection
• Virulence factor: Vi capsular antigen unique to S. typhi
• Moustache of Hydrogen sulfide (H2S) produced in TSI medium slant that
is unique finding
69.
Shigella species
• Diarrhea,+/-vomiting, fluid loss, PMNs and blood in stool
• Infection: Human to human transmission /control with good hand
hygiene
• Ingestion of low #’s of organisms make you ill [10 – 100 bacteria]
• Non lactose fermenter
• Non motile
• No Hydrogen sulfide (H2S) produced
• 4 species based on somatic (cell wall) antigen
• S. dysenteriae Group A
• S. flexneri Group B
• S. boydii Group C
• S. sonnei Group D
70.
Salmonella Shigella Agar(SS agar)
Shigella are colorless due to lactose
not being fermented. H2S produced
by Salmonella spp turning the colony
black
Hektoen agar –
Salmonella produces H2S [Hydrogen sulfide]
producing black colonies
Shigella – green colonies, no H2S produced
Normal flora – orange colored due to
fermentation of lactose (E. coli)
Non-Lactose fermenter
Shigella
Salmonella
Normal Flora
Lactose fermented
H2S
Salmonella
Shigella
Salmonella
71.
Plesiomonas shigelloides
• Foundin surface water and soil
• Pathogen of cold-blooded animals such as frogs, snakes, turtles, fish
• Associated with travel to underdeveloped countries and ingesting
contaminated water, fish, or shellfish
• Non lactose fermenter
• Oxidase enzyme positive
72.
Yersinia enterocolitica
• Majorreservoir – swine
• Humans infected by eating raw or undercooked pork
• Infections:
• Diarrhea
• Sepsis in patients with iron overload syndromes
• Mesenteric adenitis – symptomatic for right lower abdominal
pain which can be confused with appendicitis
• Sepsis from infected blood products from transfusion have
been reported
• Oxidase = negative Indole = negative
• Urease = positive Grows well at 4 °C **
• CIN agar (Cefsulodin-irgasan-novobiocin) selective agar
73.
Yersinia pestis
• CategoryA select agent, notify public health department
• Obligate flea/ rodent/ flea cycle in nature
• Human infection acquired from a rat flea bite - leads to Bubonic plague
with infection of the lymphatic system, forms painful buboes (lymph
node swelling) at site of the bite
• Hemorrhagic lymph nodes spread organism into blood stream
• Pneumonia develops following blood stream infection
• Fatality >=50%
• Endemic in SW USA
• Grows well on blood agar
• catalase +, oxidase -
• Bipolar staining looks like a “safety pin”
74.
•Vibrio cholerae
• Unsafedrinking water, poor sanitation, and inadequate
hygiene are highest risks for cholera
• Halophilic (salt loving) – salt enhances growth
• Produces Rice water diarrheal stool / mucus flecks
• Virulence due to enterotoxin production –
– Receptor on epithelial cell in small bowel –
– Activates adenyl cyclase which
– Increases cAMP with hyper secretion of NaCl and H20
– Death from dehydration and metabolic acidosis
– Curved “C” shape Gram negative rod
• Selective medium thio citrate bile sucrose agar, (TCBS) yellow
color from sucrose fermentation
• Oxidase = positive
TCBS Agar
75.
• Vibrio parahaemolyticus
•Diarrhea from ingestion of contaminated raw oysters
• Self limited in normal host, but serious in immune suppressed
• TCBS medium sucrose fermentation negative so green colony
• Vibrio vulnificus
• Skin infection from injury in contaminated water
• Diarrhea from ingestion of contaminated oysters
• Bacteremia can occur in certain patient populations following
the ingestion of contaminated oysters
• Patients with liver disease (cirrhosis) and patients with
increased serum iron
• Formation of painful skin lesions on lower extremities
with muscle necrosis
• 50% fatality rate
76.
Acinetobacter baumannii
•Environmental saprophyteand normal flora on human skin
•Gram negative coccoid-bacilli
•Does not ferment lactose / Oxidase enzyme negative
•Opportunistic nosocomial pathogen
• Glucose oxidizer
• Pulmonary infection in vented patients
• Can acquire resistance to many antibiotics from antibiotic exposure
CRAB – Carbapenemase resistant Ac. baumannii
Stenotrophomonas maltophilia
•Rapid maltose oxidizer
•Gram negative bacillus
•Gun metal gray pigment
•Intrinsically resistant to many antibiotics, including carbapenems
•Nosocomial pathogen: super-colonizer after long term carbapenem therapy due to
intrinsic resistance to the carbapenem antibiotics
Non-Fermentative Gram negative Bacilli
77.
Pseudomonas aeruginosa
• Fluorescentblue-green pigment produced (pyocyanin)
• Oxidase enzyme = positive
• Grape-like odor
• Grows at 42˚C
• Ps fluorescens/putida, related species does not grow at
42°C
• Pathogen of cystic fibrosis
• Mucoid strains produced in the lung from the production of
polysaccharide capsule
• Major lung damage results from co-infection with
Burkholderia cepacia (gram negative rod)
• Nosocomial pathogen associated with exposure to water and
moist environments, burns, swimmer’s ear, keratitis, and hot tub
folliculitis
• Intrinsically resistant to many antibiotics and can acquire
resistance to carbapenems
78.
Burkholderia pseudomallei
• Biosafetylevel 3 containment and PPE for working with the organism/
Category A select agent
• Soil-dwelling bacterium endemic in tropical and subtropical regions
worldwide, particularly in Thailand and northern Australia.
• Infects humans and livestock such as goats, pigs, and sheep and causes
the disease melioidosis which is primarily a pneumonia. Mortality is 20 –
50%
• Grows on a large variety of culture media including BAP and MacConkey
agar in 24 hours at 35* C
• Colonies are wrinkled, metallic appearance, and an earthy odor.
Burkholderia cepacia
• Primary source contaminated water
• Major pathogen of cystic fibrosis
• Grows well on most media types and produces a yellow colony
• Oxidase positive
79.
• Elizabethkingia (Chryseobacterium)meningosepticum
• Infections:
• Newborns: fatal meningitis and septicemia in the newborn
• Elderly/immune suppressed: bacteremia
• Environmental organism found in water
• Yellow colony
• Oxidase positive and Indole positive
• Haemophilus ducreyi
• Cause of venereal disease: Chancroid
• Painful necrotizing genital ulcers/inguinal lymphadenopathy
• School of fish appearance on Gram stain from lesion
• Requires hemin (X factor) to grow on solid media
80.
Haemophilus influenzae
• Transmission– close contact and secretions
• Small pleomorphic Gram negative rod
• Virulence factor – capsular polysaccharide
• Requires 2 nutritional factors for growth:
• X factor = hemin
• V factor = NAD (nicotinamide adenine dinucleotide)
• Grows on chocolate agar (contains X and V factor)
• Will not grow on 5% sheep’s blood agar
• Requires 5-8% C0₂ for growth
• Effective vaccine targets invasive infections with H. influenzae type B
(Hib) effectively eliminating most childhood invasive infections
• Ampicillin resistance from beta lactamase enzyme productions [25 %],
3rd
generation Cephalosporin becomes the antibiotic of choice for
invasive infections
Satellite
phenomenon
Staph aureus
supplies the X and V
factors required
81.
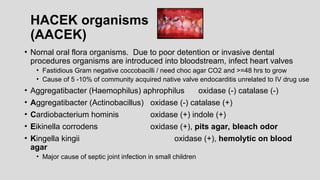
HACEK organisms
(AACEK)
• Nornaloral flora organisms. Due to poor detention or invasive dental
procedures organisms are introduced into bloodstream, infect heart valves
• Fastidious Gram negative coccobacilli / need choc agar CO2 and >=48 hrs to grow
• Cause of 5 -10% of community acquired native valve endocarditis unrelated to IV drug use
• Aggregatibacter (Haemophilus) aphrophilus oxidase (-) catalase (-)
• Aggregatibacter (Actinobacillus) oxidase (-) catalase (+)
• Cardiobacterium hominis oxidase (+) indole (+)
• Eikinella corrodens oxidase (+), pits agar, bleach odor
• Kingella kingii oxidase (+), hemolytic on blood
agar
• Major cause of septic joint infection in small children
82.
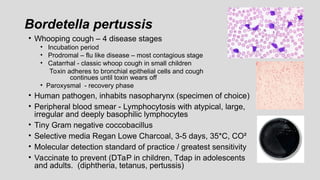
Bordetella pertussis
• Whoopingcough – 4 disease stages
• Incubation period
• Prodromal – flu like disease – most contagious stage
• Catarrhal - classic whoop cough in small children
Toxin adheres to bronchial epithelial cells and cough
continues until toxin wears off
• Paroxysmal - recovery phase
• Human pathogen, inhabits nasopharynx (specimen of choice)
• Peripheral blood smear - Lymphocytosis with atypical, large,
irregular and deeply basophilic lymphocytes
• Tiny Gram negative coccobacillus
• Selective media Regan Lowe Charcoal, 3-5 days, 35*C, CO²
• Molecular detection standard of practice / greatest sensitivity
• Vaccinate to prevent (DTaP in children, Tdap in adolescents
and adults. (diphtheria, tetanus, pertussis)
83.
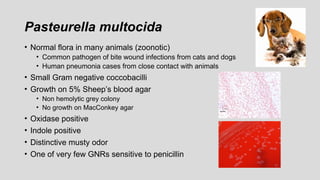
Pasteurella multocida
• Normalflora in many animals (zoonotic)
• Common pathogen of bite wound infections from cats and dogs
• Human pneumonia cases from close contact with animals
• Small Gram negative coccobacilli
• Growth on 5% Sheep’s blood agar
• Non hemolytic grey colony
• No growth on MacConkey agar
• Oxidase positive
• Indole positive
• Distinctive musty odor
• One of very few GNRs sensitive to penicillin
84.
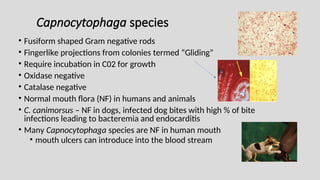
Capnocytophaga species
• Fusiformshaped Gram negative rods
• Fingerlike projections from colonies termed “Gliding”
• Require incubation in C02 for growth
• Oxidase negative
• Catalase negative
• Normal mouth flora (NF) in humans and animals
• C. canimorsus – NF in dogs, infected dog bites with high % of bite
infections leading to bacteremia and endocarditis
• Many Capnocytophaga species are NF in human mouth
• mouth ulcers can introduce into the blood stream
85.
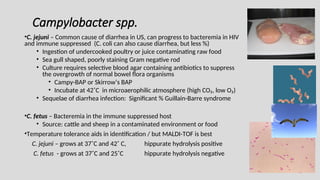
Campylobacter spp.
•C. jejuni– Common cause of diarrhea in US, can progress to bacteremia in HIV
and immune suppressed (C. coli can also cause diarrhea, but less %)
• Ingestion of undercooked poultry or juice contaminating raw food
• Sea gull shaped, poorly staining Gram negative rod
• Culture requires selective blood agar containing antibiotics to suppress
the overgrowth of normal bowel flora organisms
• Campy-BAP or Skirrow’s BAP
• Incubate at 42˚C in microaerophilic atmosphere (high CO₂, low O₂)
• Sequelae of diarrhea infection: Significant % Guillain-Barre syndrome
•C. fetus – Bacteremia in the immune suppressed host
• Source: cattle and sheep in a contaminated environment or food
•Temperature tolerance aids in identification / but MALDI-TOF is best
C. jejuni – grows at 37˚C and 42˚ C, hippurate hydrolysis positive
C. fetus - grows at 37˚C and 25˚C hippurate hydrolysis negative
86.
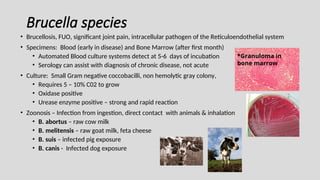
Brucella species
• Brucellosis,FUO, significant joint pain, intracellular pathogen of the Reticuloendothelial system
• Specimens: Blood (early in disease) and Bone Marrow (after first month)
• Automated Blood culture systems detect at 5-6 days of incubation
• Serology can assist with diagnosis of chronic disease, not acute
• Culture: Small Gram negative coccobacilli, non hemolytic gray colony,
• Requires 5 – 10% C02 to grow
• Oxidase positive
• Urease enzyme positive – strong and rapid reaction
• Zoonosis – Infection from ingestion, direct contact with animals & inhalation
• B. abortus – raw cow milk
• B. melitensis – raw goat milk, feta cheese
• B. suis – infected pig exposure
• B. canis - Infected dog exposure
*Granuloma in
bone marrow
87.
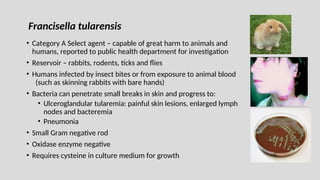
• Category ASelect agent – capable of great harm to animals and
humans, reported to public health department for investigation
• Reservoir – rabbits, rodents, ticks and flies
• Humans infected by insect bites or from exposure to animal blood
(such as skinning rabbits with bare hands)
• Bacteria can penetrate small breaks in skin and progress to:
• Ulceroglandular tularemia: painful skin lesions, enlarged lymph
nodes and bacteremia
• Pneumonia
• Small Gram negative rod
• Oxidase enzyme negative
• Requires cysteine in culture medium for growth
Francisella tularensis
88.
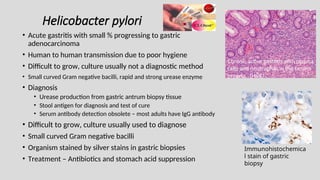
Helicobacter pylori
• Acutegastritis with small % progressing to gastric
adenocarcinoma
• Human to human transmission due to poor hygiene
• Difficult to grow, culture usually not a diagnostic method
• Small curved Gram negative bacilli, rapid and strong urease enzyme
• Diagnosis
• Urease production from gastric antrum biopsy tissue
• Stool antigen for diagnosis and test of cure
• Serum antibody detection obsolete – most adults have IgG antibody
• Difficult to grow, culture usually used to diagnose
• Small curved Gram negative bacilli
• Organism stained by silver stains in gastric biopsies
• Treatment – Antibiotics and stomach acid suppression
Immunohistochemica
l stain of gastric
biopsy
Chronic active gastritis with plasma
cells and neutrophils in the lamina
propria. (H&E)
89.
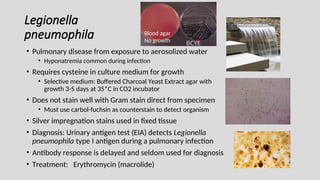
Legionella
pneumophila
• Pulmonary diseasefrom exposure to aerosolized water
• Hyponatremia common during infection
• Requires cysteine in culture medium for growth
• Selective medium: Buffered Charcoal Yeast Extract agar with
growth 3-5 days at 35*C in CO2 incubator
• Does not stain well with Gram stain direct from specimen
• Must use carbol-fuchsin as counterstain to detect organism
• Silver impregnation stains used in fixed tissue
• Diagnosis: Urinary antigen test (EIA) detects Legionella
pneumophila type I antigen during a pulmonary infection
• Antibody response is delayed and seldom used for diagnosis
• Treatment: Erythromycin (macrolide)
BCYE
Blood agar
No growth
90.
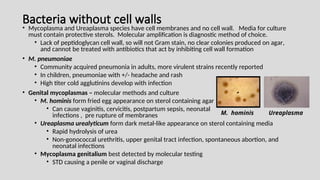
Bacteria without cellwalls
• Mycoplasma and Ureaplasma species have cell membranes and no cell wall. Media for culture
must contain protective sterols. Molecular amplification is diagnostic method of choice.
• Lack of peptidoglycan cell wall, so will not Gram stain, no clear colonies produced on agar,
and cannot be treated with antibiotics that act by inhibiting cell wall formation
• M. pneumoniae
• Community acquired pneumonia in adults, more virulent strains recently reported
• In children, pneumoniae with +/- headache and rash
• High titer cold agglutinins develop with infection
• Genital mycoplasmas – molecular methods and culture
• M. hominis form fried egg appearance on sterol containing agar
• Can cause vaginitis, cervicitis, postpartum sepsis, neonatal
infections , pre rupture of membranes
• Ureaplasma urealyticum form dark metal-like appearance on sterol containing media
• Rapid hydrolysis of urea
• Non-gonococcal urethritis, upper genital tract infection, spontaneous abortion, and
neonatal infections
• Mycoplasma genitalium best detected by molecular testing
• STD causing a penile or vaginal discharge
Ureaplasma
M. hominis
91.
Unusual and Difficultto Grow Bacteria
• Bartonella henselae
• Cat scratch disease from exposure to cat and cat excrement
• Bacillary angiomatosis – vascular skin lesions +/- invasion, associated with HIV
• Bartonella quintana – cause of trench fever/ vector is the body louse
• Coxiella burnetii – Q fever / zoonotic infection that infect humans, headache, high
fever and fatigue. Can affect heart function and can be fatal.
• Chlamydia trachomatis Serovars L1,L2,& L3
Lymphogranuloma venereum – STD that involves
lymphatics and causes enlarged lymph nodes
• Chlamydia pneumoniae (TWAR agent)- Pneumonia
• Chlamydia psittaci- psittacosis, pneumonia from exotic parrot exposure
Serologic and molecular assays for diagnosis
92.
Unusual and Difficultto Grow Bacteria
•Klebsiella (Calymmatobacterium) granulomatis
• STD disease - granuloma inguinale
• Infection leads to development of ulcerative genital lesions
•Streptobacillus moniliformis
• Rat bite fever or Haverhill fever
• Infection from untreated bite from infected rat
• Cell wall deficient bacteria known as L form
• Inhibited by SPS (anticoagulant in blood culture media) and requires serum
supplementation to grow in blood cultures
• Patient history is helpful, PCR and sequencing methods available
•Tropheryma whipplei –
• Whipple disease
• Gram positive rod (Phylum: Actinomycetota) distant relative of
Mycobacterium avium and M. paratuberculosis
• Found in soil and farm animals
• Causes a diarrhea which can lead to malabsorption syndrome and cardiac
disease
• Characteristic findings in fixed tissue
Foamy macrophages in the
lamina propria
93.
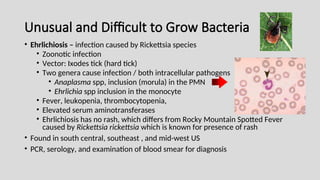
Unusual and Difficultto Grow Bacteria
• Ehrlichiosis – infection caused by Rickettsia species
• Zoonotic infection
• Vector: Ixodes tick (hard tick)
• Two genera cause infection / both intracellular pathogens
• Anaplasma spp, inclusion (morula) in the PMN
• Ehrlichia spp inclusion in the monocyte
• Fever, leukopenia, thrombocytopenia,
• Elevated serum aminotransferases
• Ehrlichiosis has no rash, which differs from Rocky Mountain Spotted Fever
caused by Rickettsia rickettsia which is known for presence of rash
• Found in south central, southeast , and mid-west US
• PCR, serology, and examination of blood smear for diagnosis
94.
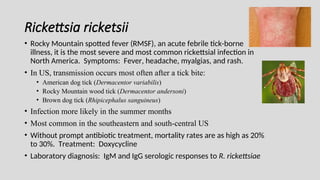
Rickettsia ricketsii
• RockyMountain spotted fever (RMSF), an acute febrile tick-borne
illness, it is the most severe and most common rickettsial infection in
North America. Symptoms: Fever, headache, myalgias, and rash.
• In US, transmission occurs most often after a tick bite:
• American dog tick (Dermacentor variabilis)
• Rocky Mountain wood tick (Dermacentor andersoni)
• Brown dog tick (Rhipicephalus sanguineus)
• Infection more likely in the summer months
• Most common in the southeastern and south-central US
• Without prompt antibiotic treatment, mortality rates are as high as 20%
to 30%. Treatment: Doxycycline
• Laboratory diagnosis: IgM and IgG serologic responses to R. rickettsiae
95.
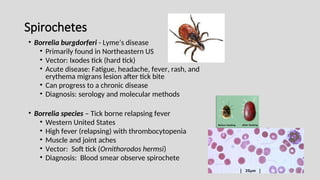
Spirochetes
• Borrelia burgdorferi- Lyme’s disease
• Primarily found in Northeastern US
• Vector: Ixodes tick (hard tick)
• Acute disease: Fatigue, headache, fever, rash, and
erythema migrans lesion after tick bite
• Can progress to a chronic disease
• Diagnosis: serology and molecular methods
• Borrelia species – Tick borne relapsing fever
• Western United States
• High fever (relapsing) with thrombocytopenia
• Muscle and joint aches
• Vector: Soft tick (Ornithorodos hermsi)
• Diagnosis: Blood smear observe spirochete
96.
Spirochetes
•Treponema pallidum
• Agentof Syphilis- A bacterial infection usually spread by sexual contact that starts
as a painless sore.
• Syphilis develops in stages, and symptoms vary with each stage.
• The first stage involves a painless sore on the genitals, rectum, or mouth. After
the initial sore heals
• The second stage is characterized by a rash. Then, there are no symptoms until
the final stage which may occur years later.
• The final stage can result in damage to the brain, nerves, eyes, or heart.
• Syphilis is treated with penicillin. Sexual partners should also be treated.
97.
Diagnosis of Syphilis
•Traditional Algorithm involves serologic screening for Syphilis using a
nontreponemal test (e.g., VDRL and RPR) first then followed by a
treponemal specific test such as EIA, TPPA, or FTA-ABS. This traditional
method has a high positive predictive value but often misses early
primary disease and treated past infections.
• New Reverse Algorithm for syphilis diagnosis consists of first
performing a treponemal antibody screening immunoassay followed by
confirmatory nontreponemal antibody testing (RPR).This algorithm was
created to increase sensitivity of detection, particularly in early stage
• Years past: Darkfield examination was used to visualize
spirochetes in lesions, replaced by PCR.
98.
Treponema pallidum subspecies
•Treponema pallidum subspecies pertenue, the agent of Yaws.
• Yaws is a chronic bacterial infection that affects the skin, bone,
and cartilage.
• Yaws most often affects children in tropical regions of Africa,
Asia, and Latin America. It spreads through direct contact with
the skin of an infected person.
• A single, berry-like sore on the skin is the first sign of yaws.
Without treatment, sores begin to spread. Yaws may eventually
cause major disfigurement and disability.
• The condition can be treated with antibiotics, azithromycin or
penicillin
99.
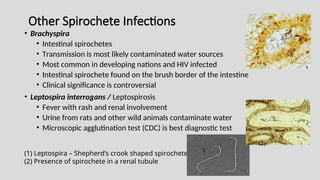
Other Spirochete Infections
•Brachyspira
• Intestinal spirochetes
• Transmission is most likely contaminated water sources
• Most common in developing nations and HIV infected
• Intestinal spirochete found on the brush border of the intestine
• Clinical significance is controversial
• Leptospira interrogans / Leptospirosis
• Fever with rash and renal involvement
• Urine from rats and other wild animals contaminate water
• Microscopic agglutination test (CDC) is best diagnostic test
(1) Leptospira – Shepherd’s crook shaped spirochete
(2) Presence of spirochete in a renal tubule
(2)
1
100.
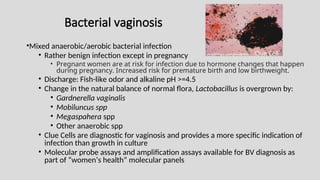
Bacterial vaginosis
•Mixed anaerobic/aerobicbacterial infection
• Rather benign infection except in pregnancy
• Pregnant women are at risk for infection due to hormone changes that happen
during pregnancy. Increased risk for premature birth and low birthweight.
• Discharge: Fish-like odor and alkaline pH >=4.5
• Change in the natural balance of normal flora, Lactobacillus is overgrown by:
• Gardnerella vaginalis
• Mobiluncus spp
• Megaspahera spp
• Other anaerobic spp
• Clue Cells are diagnostic for vaginosis and provides a more specific indication of
infection than growth in culture
• Molecular probe assays and amplification assays available for BV diagnosis as
part of “women’s health” molecular panels
Clue Cell
101.
Anaerobic Bacteria
• Anaerobicinfections can occur in virtually any organ or region of
the body
• Most are polymicrobial –with both aerobic and anaerobic species
• Endogenous normal flora organisms cause most infections
• Due to trauma, vascular or tissue necrosis, there is a lowered oxygen
supply to the involved tissue that can lead to anaerobe proliferation
• Treatment: Surgery to restore oxygen to tissue, remove necrotic
tissue and antimicrobial therapy
• Specimen collection for culture
• Gel containing swab / gel protective against oxygen
• Eswab - immersion into broth / stability for <=24 hrs
• Evacuated vials (port-o-cult)/ oxygen free vials for fluids
• Do not refrigerate specimen prior to culture, leads to greater
absorption of oxygen and decrease viability of anaerobic species
102.
Anaerobic culture
• PRASmedia – pre reduced anaerobically sterile
• Media packaged in oxygen free environment
• Provides good environment for growth of anaerobes
• Most common anaerobic culture media include:
• CDC anaerobic enriched Sheep”s blood agar
• Kanamycin-vancomycin blood agar
• Bile esculin agar
• Thioglycolate broth
• Chopped meat glucose broth
• Anaerobic chambers – Culture workup performed in an oxygen free closed
cabinet, specimens and organisms are never exposed to oxygen
• Anaerobic gas packs and jars for anaerobic incubation of culture plates
• Wet pack – 10 ml water added to hydrogen and CO2 generating
envelope/ requires palladium coated catalyst in jar lid to generate heat
and activate oxygen free environment.
• Dry pack – (Anaeropack) absorbs O2 and generates CO2
PRAS
103.
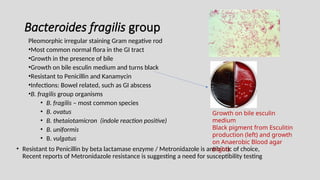
Bacteroides fragilis group
Pleomorphicirregular staining Gram negative rod
•Most common normal flora in the GI tract
•Growth in the presence of bile
•Growth on bile esculin medium and turns black
•Resistant to Penicillin and Kanamycin
•Infections: Bowel related, such as GI abscess
•B. fragilis group organisms
• B. fragilis – most common species
• B. ovatus
• B. thetaiotamicron (indole reaction positive)
• B. uniformis
• B. vulgatus
• Resistant to Penicillin by beta lactamase enzyme / Metronidazole is antibiotic of choice,
Recent reports of Metronidazole resistance is suggesting a need for susceptibility testing
Growth on bile esculin
medium
Black pigment from Esculitin
production (left) and growth
on Anaerobic Blood agar
(right)
104.
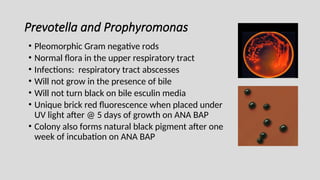
Prevotella and Prophyromonas
•Pleomorphic Gram negative rods
• Normal flora in the upper respiratory tract
• Infections: respiratory tract abscesses
• Will not grow in the presence of bile
• Will not turn black on bile esculin media
• Unique brick red fluorescence when placed under
UV light after @ 5 days of growth on ANA BAP
• Colony also forms natural black pigment after one
week of incubation on ANA BAP
105.
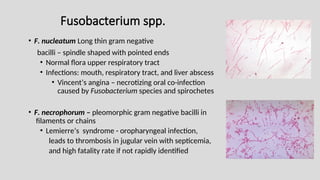
Fusobacterium spp.
• F.nucleatum Long thin gram negative
bacilli – spindle shaped with pointed ends
• Normal flora upper respiratory tract
• Infections: mouth, respiratory tract, and liver abscess
• Vincent’s angina – necrotizing oral co-infection
caused by Fusobacterium species and spirochetes
• F. necrophorum – pleomorphic gram negative bacilli in
filaments or chains
• Lemierre’s syndrome - oropharyngeal infection,
leads to thrombosis in jugular vein with septicemia,
and high fatality rate if not rapidly identified
106.
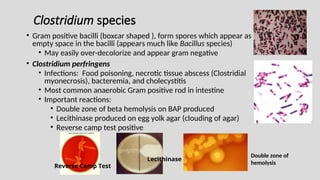
Clostridium species
• Grampositive bacilli (boxcar shaped ), form spores which appear as
empty space in the bacilli (appears much like Bacillus species)
• May easily over-decolorize and appear gram negative
• Clostridium perfringens
• Infections: Food poisoning, necrotic tissue abscess (Clostridial
myonecrosis), bacteremia, and cholecystitis
• Most common anaerobic Gram positive rod in intestine
• Important reactions:
• Double zone of beta hemolysis on BAP produced
• Lecithinase produced on egg yolk agar (clouding of agar)
• Reverse camp test positive
Lecithinase
Reverse Camp Test
Double zone of
hemolysis
107.
• Clostridium botulinum– Botulism
• Adult disease – ingest preformed heat labile neurotoxin,
from ingestion of mass produced or
home canned foods
• Infant disease - spore ingested from nature (household
dust) or product of nature such as honey. The spores
germinate in gut producing neurotoxin.
• Begins with constipation and difficult sucking bottle
• Both forms are life threatening neuroparalytic diseases
• Clostridium tetani - Tetanus
• Gram stained cells appear like Tennis racket from
terminal spore production
• Infection begins with a penetrating skin injury that
introduces the Tetanospasmin toxin into tissue
• Spastic contractions of voluntary muscles, hyper-
reflexia, lock jaw (trismus)
• DTaP vaccine to prevent (Diphtheria, Tetanus, Pertussis)
108.
• Clostridium septicum–
• Bacteremia or gas gangrene in patient with underlying malignancy
• Hematogenous spread from GI tract leads to bacteremia – no trauma necessary
• Clostridioides (Clostridium) difficile –
• Disease: antibiotic associated colitis, intestinal pseudo-membranes can be produced
• Toxin A – enterotoxin causes fluid accumulation
• Toxin B – potent cell cytotoxin, primary virulence factor (TcdB gene)
• Binary toxin – Nap1 strain, increased toxin production, with more serious disease
• Diagnosis of infection: Only test diarrhetic stools, do not test hard stools
• Standard of practice for C. difficile disease diagnosis has become a two-step algorithm:
• Step 1: Molecular amplification for toxin gene in the stool (TcdB gene)
• Step 2: Enzyme immunoassay to detect active toxin in the stool
• If TcdB gene and toxin both detected, patient has C. difficile infection and requires therapy
• If only the TcdB gene is detected, patient is most likely only colonized and does not need therapy.
• Alternate method: GDH (Glutamate dehydrogenase) antigen test uses specific antibodies to search for the
presence of GDH, a protein present in all C. difficile isolates. Screening test with good sensitivity, rapid
turnaround time, and low cost. Detects both colonization and infection.
109.
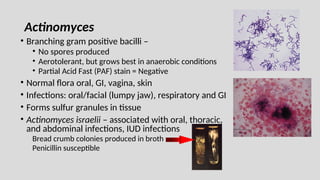
Actinomyces
• Branching grampositive bacilli –
• No spores produced
• Aerotolerant, but grows best in anaerobic conditions
• Partial Acid Fast (PAF) stain = Negative
• Normal flora oral, GI, vagina, skin
• Infections: oral/facial (lumpy jaw), respiratory and GI
• Forms sulfur granules in tissue
• Actinomyces israelii – associated with oral, thoracic,
and abdominal infections, IUD infections
Bread crumb colonies produced in broth
Penicillin susceptible
110.
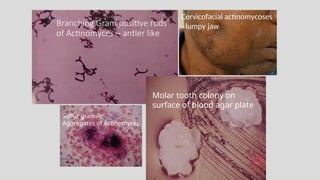
Branching Gram positiverods
of Actinomyces – antler like
Molar tooth colony on
surface of blood agar plate
Sulfur granule
Aggregates of Actinomyces
Cervicofacial actinomycoses
–lumpy jaw
111.
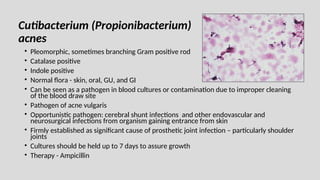
Cutibacterium (Propionibacterium)
acnes
• Pleomorphic,sometimes branching Gram positive rod
• Catalase positive
• Indole positive
• Normal flora - skin, oral, GU, and GI
• Can be seen as a pathogen in blood cultures or contamination due to improper cleaning
of the blood draw site
• Pathogen of acne vulgaris
• Opportunistic pathogen: cerebral shunt infections and other endovascular and
neurosurgical infections from organism gaining entrance from skin
• Firmly established as significant cause of prosthetic joint infection – particularly shoulder
joints
• Cultures should be held up to 7 days to assure growth
• Therapy - Ampicillin
112.
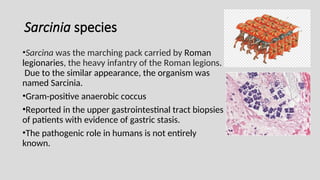
Sarcinia species
•Sarcina wasthe marching pack carried by Roman
legionaries, the heavy infantry of the Roman legions.
Due to the similar appearance, the organism was
named Sarcinia.
•Gram-positive anaerobic coccus
•Reported in the upper gastrointestinal tract biopsies
of patients with evidence of gastric stasis.
•The pathogenic role in humans is not entirely
known.





![Streptococcus pyogenes
• Group A Streptococcus [GAS] – of 5% Sheep’s blood agar produces
an intense ring of beta hemolysis around a small grey colony
• Biochemical tests used for identification:
• Bacitracin KB sensitivity test – GAS is inhibited by antibiotic
Bacitracin (A) producing a small zone of inhibition
• Not specific for GAS, inhibition also occurs with Beta hemolytic
Streptococcus group C, test is seldom used
• PYR (pyrrolidonyl arylmidase) reaction
• Organism spotted onto moist PYR disk
• Wait 2 min – room temperature incubation
• Add cinnamaldehyde reagent
• Pink = positive = Streptococcus pyogenes
• **This test is not exclusive for Strep pyogenes –
Enterococcus and Staph lugdunensis also test positive
• Therapy : Penicillin, Amoxicillin or Cephalosporin antibiotics
No resistance reported to these agents
PYR reaction
+ --](https://image.slidesharecdn.com/webbacteriology2025-250320180358-f193e766/85/WEB-BACTERIOLOGY-2025-Margie-Morgan-PhD-25-320.jpg)
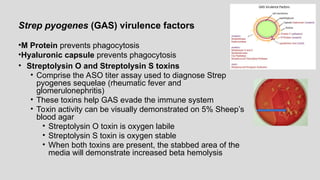
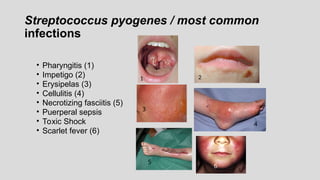
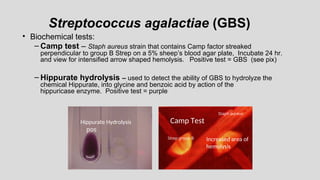
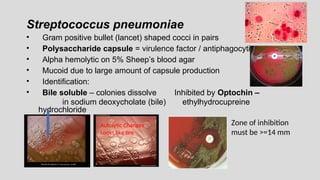
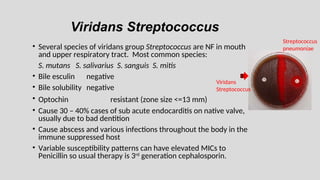
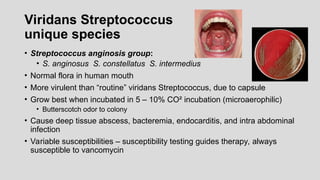
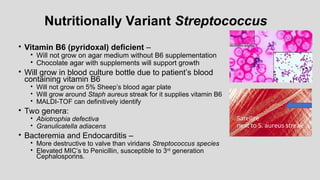
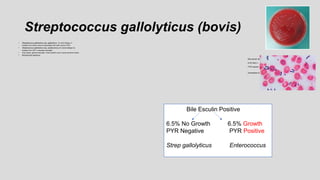
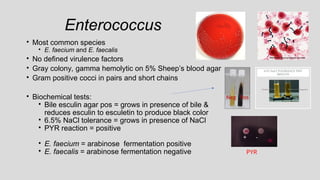

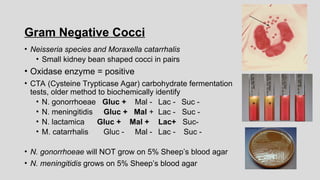
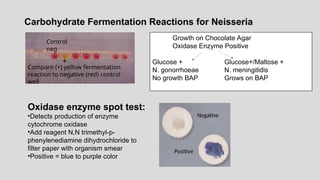
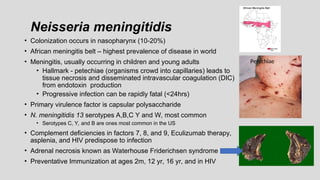
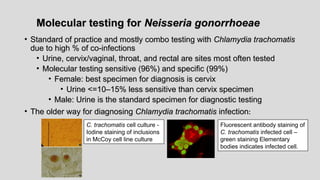
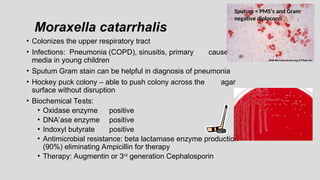
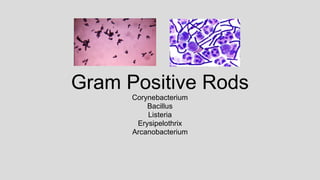
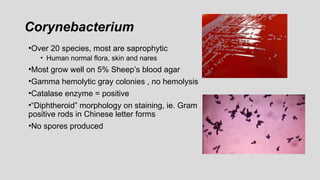
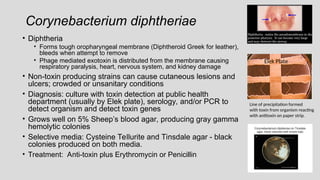
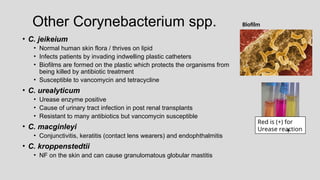
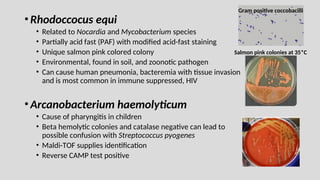
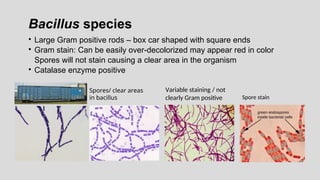
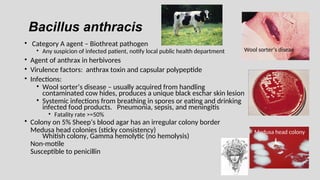
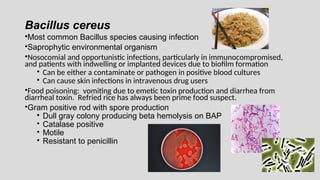
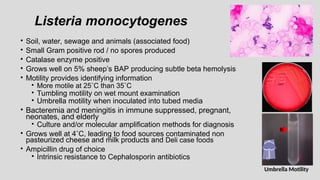
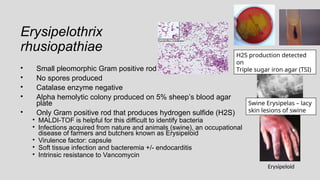
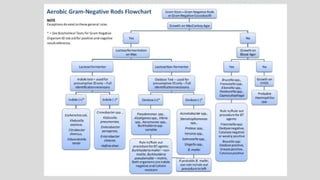
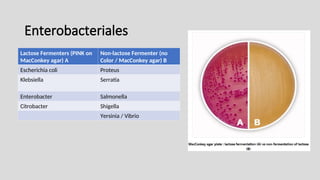
![Triple Sugar Iron Agar (TSI)– used to detect fermentation of glucose,
lactose and/or sucrose and production of hydrogen sulfide [H2S] in Gram negative
bacilli
CHO
Fermentation=
Yellow medium
Gas production=
Disruption of the
agar
No CHO
fermentation =
Red medium
H2S production
= black medium
at bottom of
tube
Pseudomonas Shigella E. coli Citrobacter Salmonella](https://image.slidesharecdn.com/webbacteriology2025-250320180358-f193e766/85/WEB-BACTERIOLOGY-2025-Margie-Morgan-PhD-60-320.jpg)
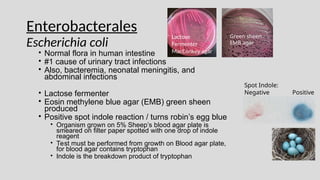
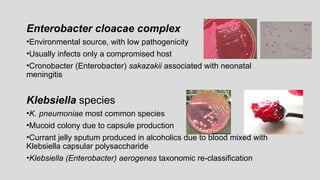
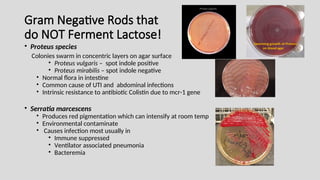
![• Salmonella species
• Diarrhea with +/- fever and PMNs in the stool
• Infection from eating contaminated food (raw eggs, poultry, ground
beef or dairy) or direct contact with a sick person or animal
– Must ingest large #’s of organisms to make you ill, normal levels
of stomach acid is protective
• MacConkey agar - does not ferment lactose
• Produces hydrogen sulfide on selective media
• Motile
• Identification based on biochemical reactions and serologic typing
• Kaufman White serologic typing for speciation of Salmonella
• O Somatic (cell wall) antigen – Salmonella group “B”
• H flagellar antigens – 2 phases [h1 & h2]
• Vi capsular antigen – Salmonella typhi only](https://image.slidesharecdn.com/webbacteriology2025-250320180358-f193e766/85/WEB-BACTERIOLOGY-2025-Margie-Morgan-PhD-67-320.jpg)
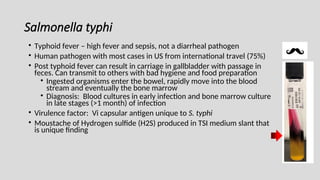
![Shigella species
• Diarrhea, +/-vomiting, fluid loss, PMNs and blood in stool
• Infection: Human to human transmission /control with good hand
hygiene
• Ingestion of low #’s of organisms make you ill [10 – 100 bacteria]
• Non lactose fermenter
• Non motile
• No Hydrogen sulfide (H2S) produced
• 4 species based on somatic (cell wall) antigen
• S. dysenteriae Group A
• S. flexneri Group B
• S. boydii Group C
• S. sonnei Group D](https://image.slidesharecdn.com/webbacteriology2025-250320180358-f193e766/85/WEB-BACTERIOLOGY-2025-Margie-Morgan-PhD-69-320.jpg)
![Salmonella Shigella Agar (SS agar)
Shigella are colorless due to lactose
not being fermented. H2S produced
by Salmonella spp turning the colony
black
Hektoen agar –
Salmonella produces H2S [Hydrogen sulfide]
producing black colonies
Shigella – green colonies, no H2S produced
Normal flora – orange colored due to
fermentation of lactose (E. coli)
Non-Lactose fermenter
Shigella
Salmonella
Normal Flora
Lactose fermented
H2S
Salmonella
Shigella
Salmonella](https://image.slidesharecdn.com/webbacteriology2025-250320180358-f193e766/85/WEB-BACTERIOLOGY-2025-Margie-Morgan-PhD-70-320.jpg)
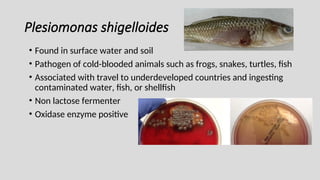
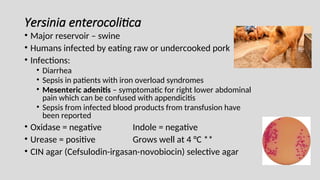
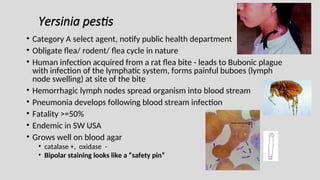
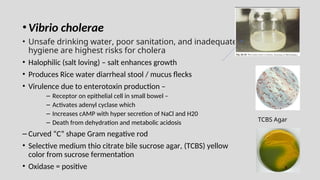
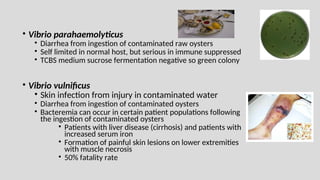
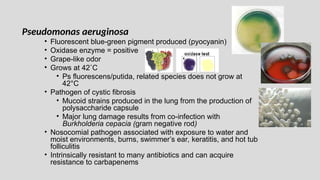
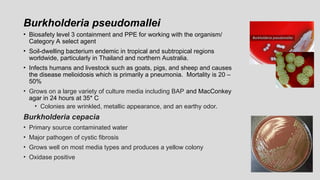
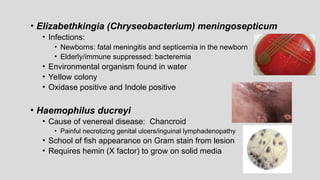
![Haemophilus influenzae
• Transmission – close contact and secretions
• Small pleomorphic Gram negative rod
• Virulence factor – capsular polysaccharide
• Requires 2 nutritional factors for growth:
• X factor = hemin
• V factor = NAD (nicotinamide adenine dinucleotide)
• Grows on chocolate agar (contains X and V factor)
• Will not grow on 5% sheep’s blood agar
• Requires 5-8% C0₂ for growth
• Effective vaccine targets invasive infections with H. influenzae type B
(Hib) effectively eliminating most childhood invasive infections
• Ampicillin resistance from beta lactamase enzyme productions [25 %],
3rd
generation Cephalosporin becomes the antibiotic of choice for
invasive infections
Satellite
phenomenon
Staph aureus
supplies the X and V
factors required](https://image.slidesharecdn.com/webbacteriology2025-250320180358-f193e766/85/WEB-BACTERIOLOGY-2025-Margie-Morgan-PhD-80-320.jpg)