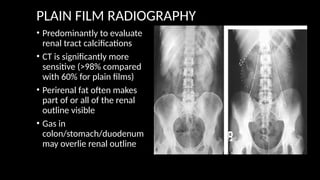
PLAIN FILM RADIOGRAPHY
•Predominantly to evaluate
renal tract calcifications
• CT is significantly more
sensitive (>98% compared
with 60% for plain films)
• Perirenal fat often makes
part of or all of the renal
outline visible
• Gas in
colon/stomach/duodenum
may overlie renal outline
4.
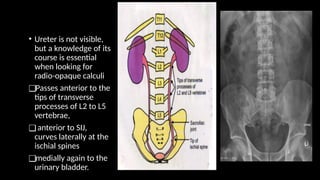
• Ureter isnot visible,
but a knowledge of its
course is essential
when looking for
radio-opaque calculi
❑Passes anterior to the
tips of transverse
processes of L2 to L5
vertebrae,
❑anterior to SIJ,
curves laterally at the
ischial spines
❑medially again to the
urinary bladder.
5.
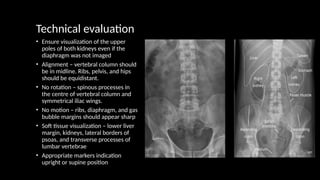
Technical evaluation
• Ensurevisualization of the upper
poles of both kidneys even if the
diaphragm was not imaged
• Alignment – vertebral column should
be in midline. Ribs, pelvis, and hips
should be equidistant.
• No rotation – spinous processes in
the centre of vertebral column and
symmetrical iliac wings.
• No motion – ribs, diaphragm, and gas
bubble margins should appear sharp
• Soft tissue visualization – lower liver
margin, kidneys, lateral borders of
psoas, and transverse processes of
lumbar vertebrae
• Appropriate markers indication
upright or supine position
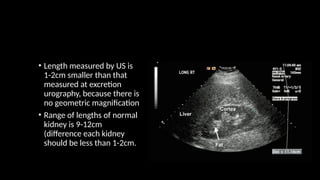
• Length measuredby US is
1-2cm smaller than that
measured at excretion
urography, because there is
no geometric magnification
• Range of lengths of normal
kidney is 9-12cm
(difference each kidney
should be less than 1-2cm.
11.
Computed tomography
INDICATIONS:
• Renalcolic/renal stone disease
• Renal tumour
• Renal/perirenal collection
• Loin mass
• Staging and follow up of urinary tract malignancy
• Investigation of renal tract obstruction
• CTA to assess renal vessels for suspected renal artery stenosis or
arterio-venous fistula/malformation, active bleeding
12.
TECHNIQUES: STANDARD DIAGNOSTICCT
• Venous access is obtained
• Patient lies supine
• Scanogram is taken of chest, abdomen, and pelvis as appropriate
• 100ml IV LOCM given
• Scans obtained approximately 70s (portal venous phase) after IV
contrast
13.
Techniques: renal lesioncharacterization
• Used to assess renal cysts or masses identified on another imaging
modality such as ultrasound
• Pre and post IV contrast scans are obtained through the kidneys in
order to assess precontrast attenuation and subsequent
enhancement patterns
14.
• Plain CTis useful to assess possible stone disease
• Used in most centres as the primary investigation of renal colic
(replacing plain KUB radiograph)
• No IV or oral contrast is given
• Patient supine
• Scan from top of the kidneys to the bladder base
15.
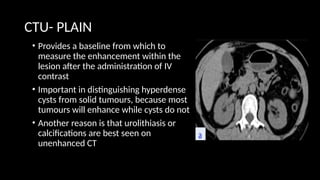
CTU- PLAIN
• Providesa baseline from which to
measure the enhancement within the
lesion after the administration of IV
contrast
• Important in distinguishing hyperdense
cysts from solid tumours, because most
tumours will enhance while cysts do not
• Another reason is that urolithiasis or
calcifications are best seen on
unenhanced CT
16.
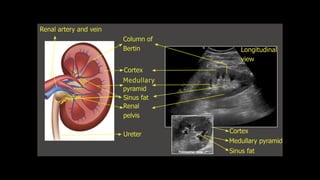
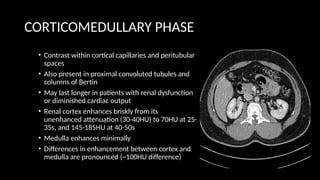
CORTICOMEDULLARY PHASE
• Contrastwithin cortical capillaries and peritubular
spaces
• Also present in proximal convoluted tubules and
columns of Bertin
• May last longer in patients with renal dysfunction
or diminished cardiac output
• Renal cortex enhances briskly from its
unenhanced attenuation (30-40HU) to 70HU at 25-
35s, and 145-185HU at 40-50s
• Medulla enhances minimally
• Differences in enhancement between cortex and
medulla are pronounced (~100HU difference)
17.
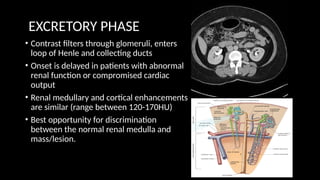
EXCRETORY PHASE
• Contrastfilters through glomeruli, enters
loop of Henle and collecting ducts
• Onset is delayed in patients with abnormal
renal function or compromised cardiac
output
• Renal medullary and cortical enhancements
are similar (range between 120-170HU)
• Best opportunity for discrimination
between the normal renal medulla and
mass/lesion.
18.
CT RENAL 4PHASE
• Positioning – supine, arm positioned comfortably above head
• Topogram – craniocaudal, in inspiration
• IV contrast
• 80ml at 4ml/sec
• Ultravist 300 (LOCM – iopromide)
• Dose
• kV:120
• Effective mAs: autocalculated by machine depending on patient’s body
habitus
19.
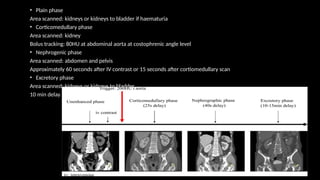
• Plain phase
Areascanned: kidneys or kidneys to bladder if haematuria
• Corticomedullary phase
Area scanned: kidney
Bolus tracking: 80HU at abdominal aorta at costophrenic angle level
• Nephrogenic phase
Area scanned: abdomen and pelvis
Approximately 60 seconds after IV contrast or 15 seconds after cortiomedullary scan
• Excretory phase
Area scanned: kidneys or kidneys to bladder
10 min delay
20.
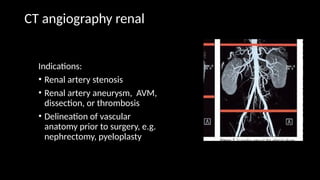
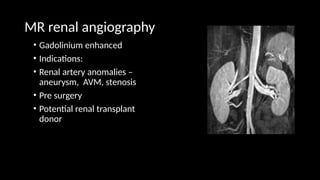
CT angiography renal
Indications:
•Renal artery stenosis
• Renal artery aneurysm, AVM,
dissection, or thrombosis
• Delineation of vascular
anatomy prior to surgery, e.g.
nephrectomy, pyeloplasty
21.
• No oraliodinated contrast used
• Scan from upper pole of kidneys to the aortic bifurcation
• Narrow collimation (1mm)
• 100-150ml of IV contrast injected at 3-4ml/sec
• Use of bolus tracking/triggering devices or timing test injections is
recommended to ensure appropriate timing
22.
MRU
Indication:
• To demonstratethe collecting system/determine level of obstruction
in a poorly functioning/obstructed kidney
• Urinary tract obstruction unrelated to urolithiasis
• Congenital anomalies
• Renal transplant donor assessment (combined with MR angiography)
23.
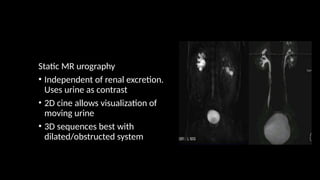
Static MR urography
•Independent of renal excretion.
Uses urine as contrast
• 2D cine allows visualization of
moving urine
• 3D sequences best with
dilated/obstructed system
24.
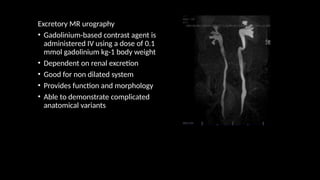
Excretory MR urography
•Gadolinium-based contrast agent is
administered IV using a dose of 0.1
mmol gadolinium kg-1 body weight
• Dependent on renal excretion
• Good for non dilated system
• Provides function and morphology
• Able to demonstrate complicated
anatomical variants
Renal scintigraphy
❑Static renalradionuclide scintigraphy
• Also known as renal cortical scan
• DMSA scan
❑Dynamic renal radionuclide scintigraphy
• Also known as renal perfusion scan
• MAG3, DTPA scan
27.
STATIC RENAL RADIONUCLIDESCINTIGRAPHY
Indications
• Assessment of individual and relative renal function
• Investigation of urinary tract infections, particularly in children for scarring
• Assessment of reflux nephropathy for scarring
• Identification of horseshoe, solitary, or ectopic kidney
• Differentiation of a pseudotumour due to hypertrophied column of Bertin from
a true tumour
Contraindication
• Pregnancy
28.
Radiopharmaceuticals
• 99m
TC-dimercaptosuccinic acid(DMSA), 80 MBq max (0.7 mSv ED)
• Bound to plasma proteins
• Cleared by tubular absorption
• DMSA is retained in the renal cortex, with an uptake of 40%-65%
of the injected dose within 2H and no significant excretion during
the imaging period
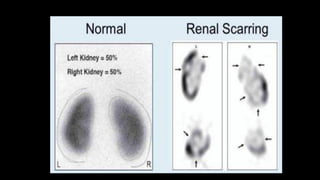
• Gives the best morphological images of any renal
radiopharmaceutical, and is used for assessment of scarring
• Gives the most accurate assessment of differential renal function
29.
Equipment
• Gamma-camera witha low-energy,
high resolution collimator
• Technique
• Radiopharmaceutical is administered
IV
• Images acquired at anytime 1-6H later
(imaging in the first hour is to be
avoided because of free 99mTC in the
urine)
30.
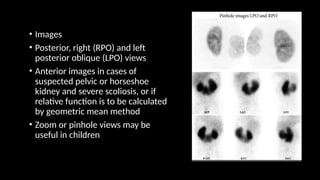
• Images
• Posterior,right (RPO) and left
posterior oblique (LPO) views
• Anterior images in cases of
suspected pelvic or horseshoe
kidney and severe scoliosis, or if
relative function is to be calculated
by geometric mean method
• Zoom or pinhole views may be
useful in children
32.
DYNAMIC RENAL RADIONUCLIDESCINTIGRAPHY
Indications
• Evaluation of obstruction
• Assessment of renal function following drainage procedures to the urinary tract
• Assessment of perfusion in acute native or transplant kidney failure
• Demonstration of vesicoureteric reflux
• Renal trauma
• Diagnosis of renal artery stenosis
• Contraindication
• None
33.
• Radiopharmaceuticals
• 99mTc-MAG-3(mercaptoacetyltriglycine)
• 100MBq max (0.7mSv ED)
• Highly protein bound
• 80% cleared by tubular secretion
• 20% by glomerular filtration
• Radiopharmaceutical of choice – better image quality, particularly in patients with
impaired renal function
• 99mTc-diethylene triamine-pentaceticacid (DTPA)
• 150MBq typical (1mSv ED)
• Cleared by glomerular filtration
• Poorer image quality due to lower kidney/background ration
34.
• Equipment
• Gamma-camerawith a low-energy general
purpose collimator
• Preparation
• Patient should be well hydrated with
around 500ml of fluid immediately before
administration of tracer
• Bladder should be voided before injection
35.
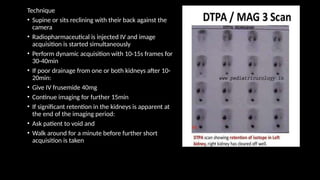
Technique
• Supine orsits reclining with their back against the
camera
• Radiopharmaceutical is injected IV and image
acquisition is started simultaneously
• Perform dynamic acquisition with 10-15s frames for
30-40min
• If poor drainage from one or both kidneys after 10-
20min:
• Give IV frusemide 40mg
• Continue imaging for further 15min
• If significant retention in the kidneys is apparent at
the end of the imaging period:
• Ask patient to void and
• Walk around for a minute before further short
acquisition is taken
RENAL ARTERIOGRAPHY
INDICATIONS
• Renalartery stenosis prior to angioplasty or stent placement
• Diagnostic arteriography has been replaced generally by MRA or CTA
• Assessment of living related renal transplant donors
• Replaced generally by MRA or CTA
• Embolization of vascular renal tumour prior to surgery
• Haematuria particularly following trauma, including biopsy
• Prior to prophylactic embolization of an angiomyolipoma (AML)
or therapeutic embolization of a bleeding AML
38.
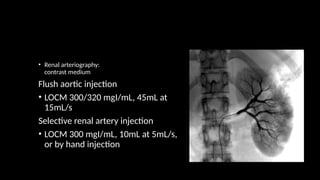
• Renal arteriography:
contrastmedium
Flush aortic injection
• LOCM 300/320 mgI/mL, 45mL at
15mL/s
Selective renal artery injection
• LOCM 300 mgI/mL, 10mL at 5mL/s,
or by hand injection
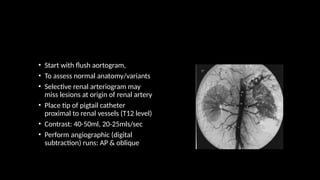
• Start withflush aortogram,
• To assess normal anatomy/variants
• Selective renal arteriogram may
miss lesions at origin of renal artery
• Place tip of pigtail catheter
proximal to renal vessels (T12 level)
• Contrast: 40-50ml, 20-25mls/sec
• Perform angiographic (digital
subtraction) runs: AP & oblique
41.
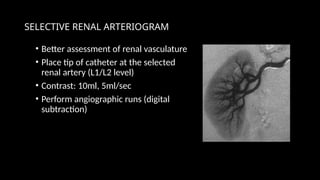
SELECTIVE RENAL ARTERIOGRAM
•Better assessment of renal vasculature
• Place tip of catheter at the selected
renal artery (L1/L2 level)
• Contrast: 10ml, 5ml/sec
• Perform angiographic runs (digital
subtraction)
42.
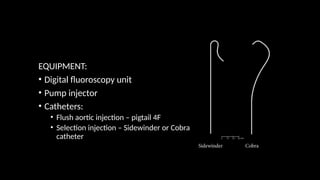
INTERVENTIONAL RADIOLOGY
• Canbe done under fluoroscopy, ultrasound, CT, and angiography
• Percutaneous renal biopsy
• Percutaneous nephrostomy
43.
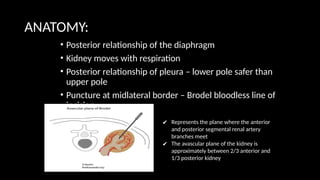
ANATOMY:
• Posterior relationshipof the diaphragm
• Kidney moves with respiration
• Posterior relationship of pleura – lower pole safer than
upper pole
• Puncture at midlateral border – Brodel bloodless line of
incision
✔ Represents the plane where the anterior
and posterior segmental renal artery
branches meet
✔ The avascular plane of the kidney is
approximately between 2/3 anterior and
1/3 posterior kidney
44.
PERCUTANEOUS RENAL BIOPSY
Indication
•Diagnostic biopsy: unexplained renal failure, mass
Contraindication
• Bleeding diathesis
Equipment
• USG or CT guidance
• Bard gun with core biopsy needle
Patient preparation
• Fasting for 4 hours
• Blood parameters
• Premedication/sedation as required
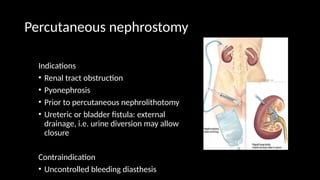
Percutaneous nephrostomy
Indications
• Renaltract obstruction
• Pyonephrosis
• Prior to percutaneous nephrolithotomy
• Ureteric or bladder fistula: external
drainage, i.e. urine diversion may allow
closure
Contraindication
• Uncontrolled bleeding diasthesis
48.
• Contrast medium
•LOCM
• Equipment
• Puncture needle/coaxial needle
• Drainage catheter
• J-guidewire
• USG and/or fluoroscopy
• Patient preparation
• Fasting for 4 hours
• Blood parameters
• Premedication/sedation as required
• May need prophylactic antibiotics
49.
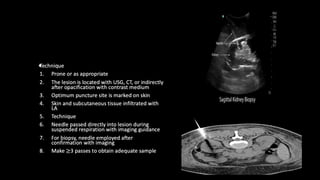
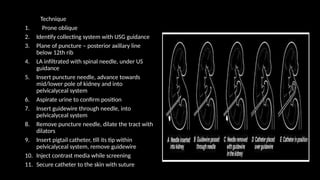
Technique
1. Prone oblique
2.Identify collecting system with USG guidance
3. Plane of puncture – posterior axillary line
below 12th rib
4. LA infiltrated with spinal needle, under US
guidance
5. Insert puncture needle, advance towards
mid/lower pole of kidney and into
pelvicalyceal system
6. Aspirate urine to confirm position
7. Insert guidewire through needle, into
pelvicalyceal system
8. Remove puncture needle, dilate the tract with
dilators
9. Insert pigtail catheter, till its tip within
pelvicalyceal system, remove guidewire
10. Inject contrast media while screening
11. Secure catheter to the skin with suture
50.
Complications
• Septicemia
• Hemorrhage
•Perforation of collecting system with urine leak
• Unsuccessful drainage
• Injury to adjacent organs
• Catheter dislodgement