Downloaded 1,189 times

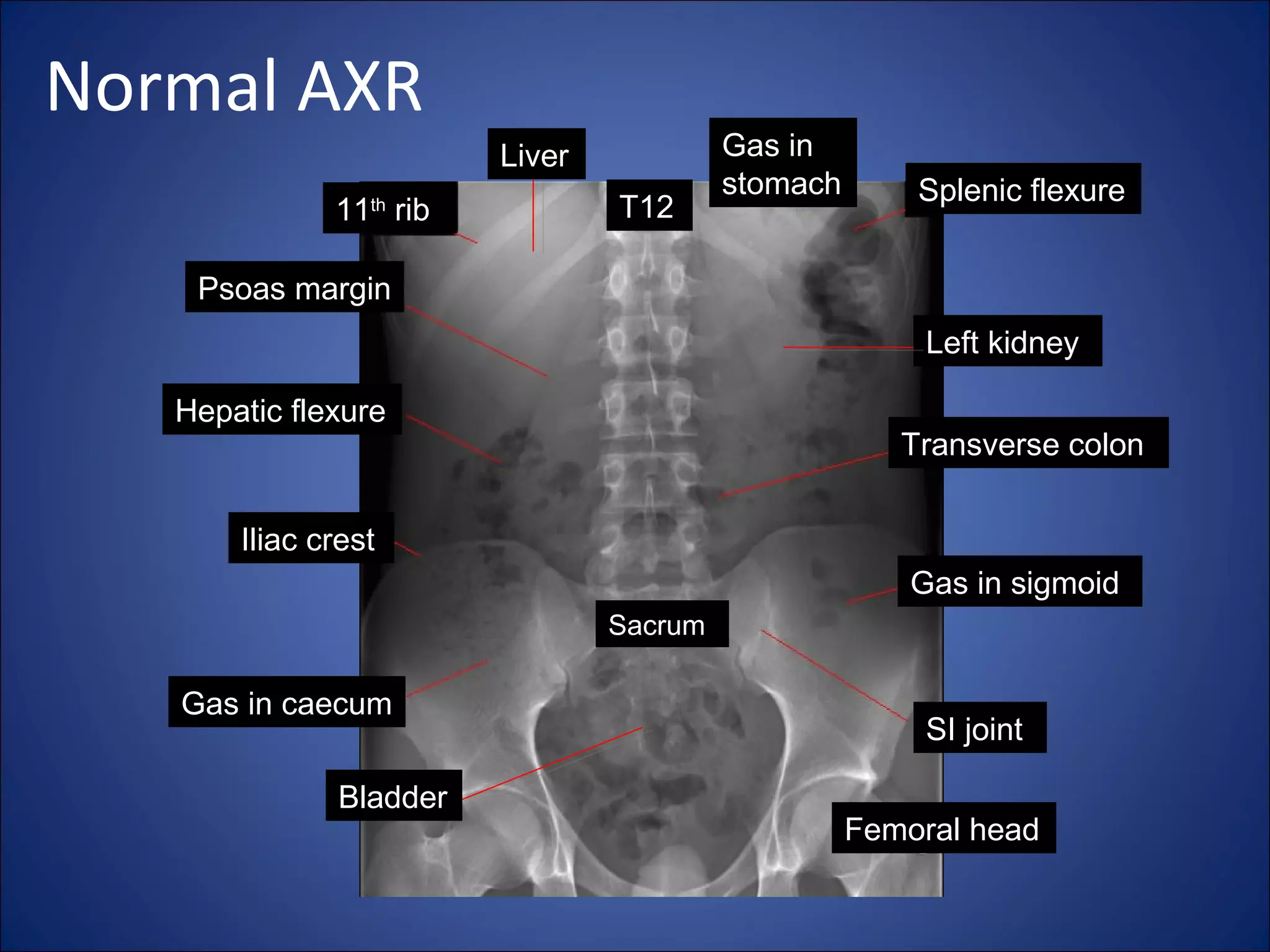
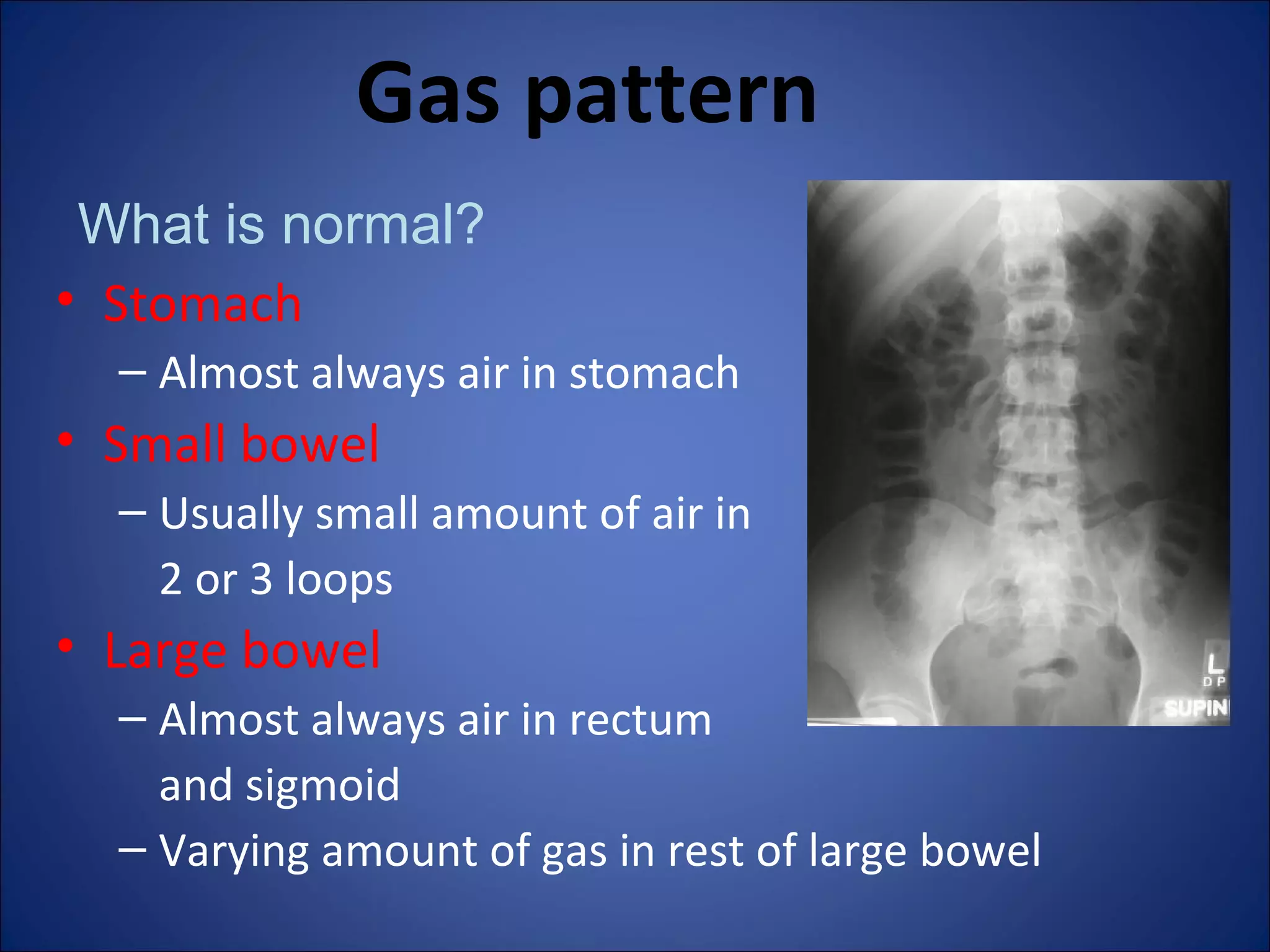
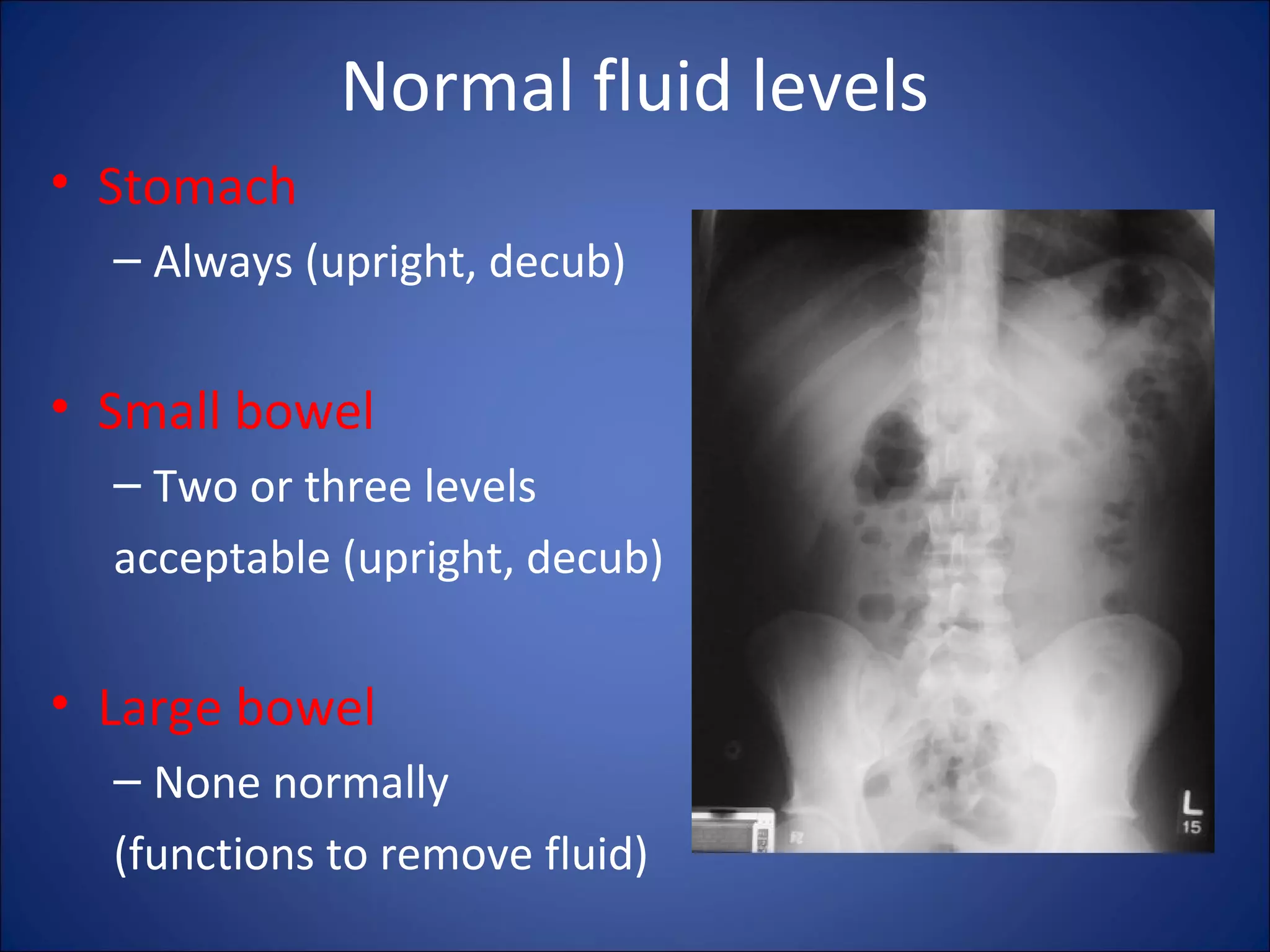
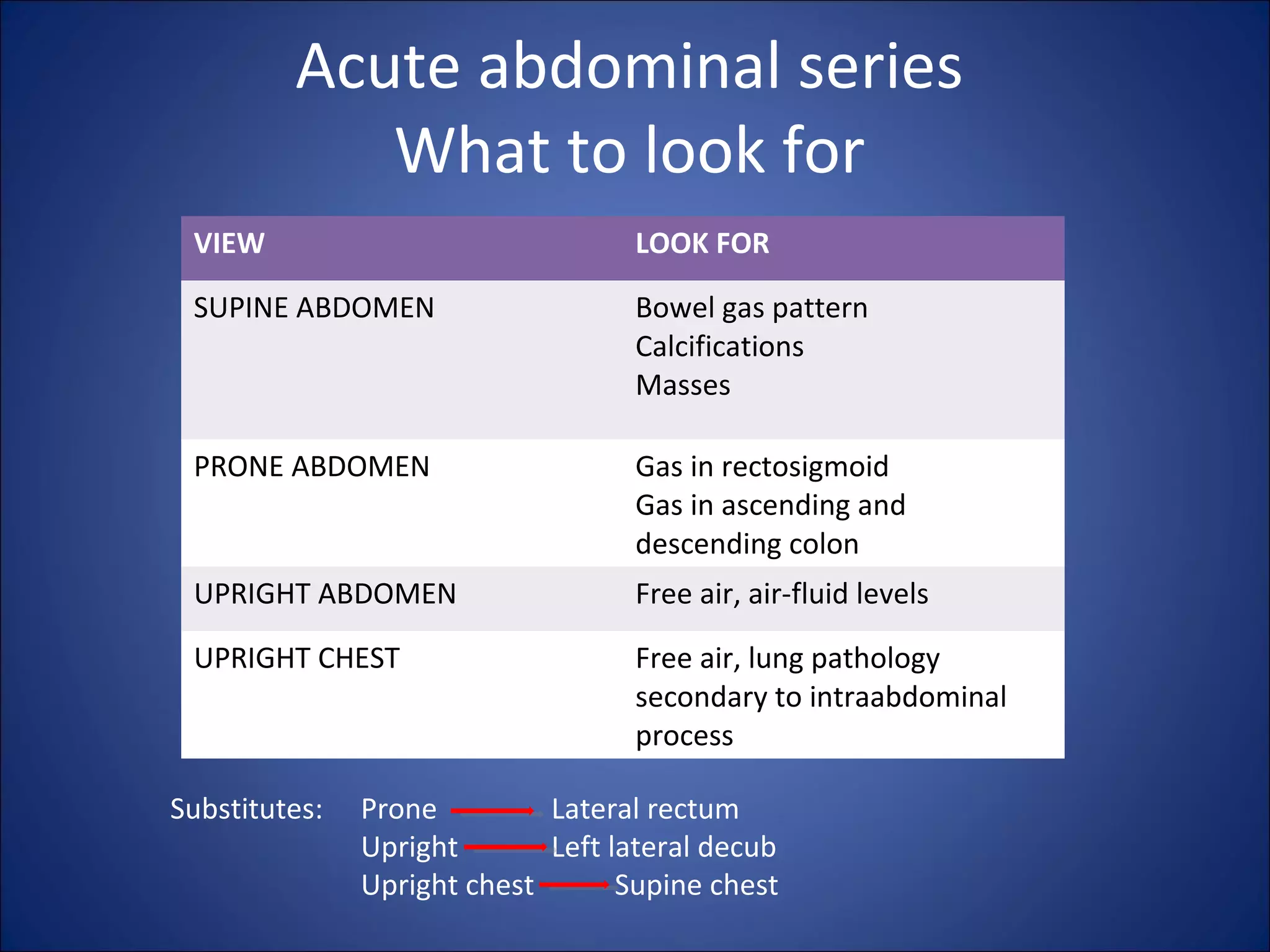







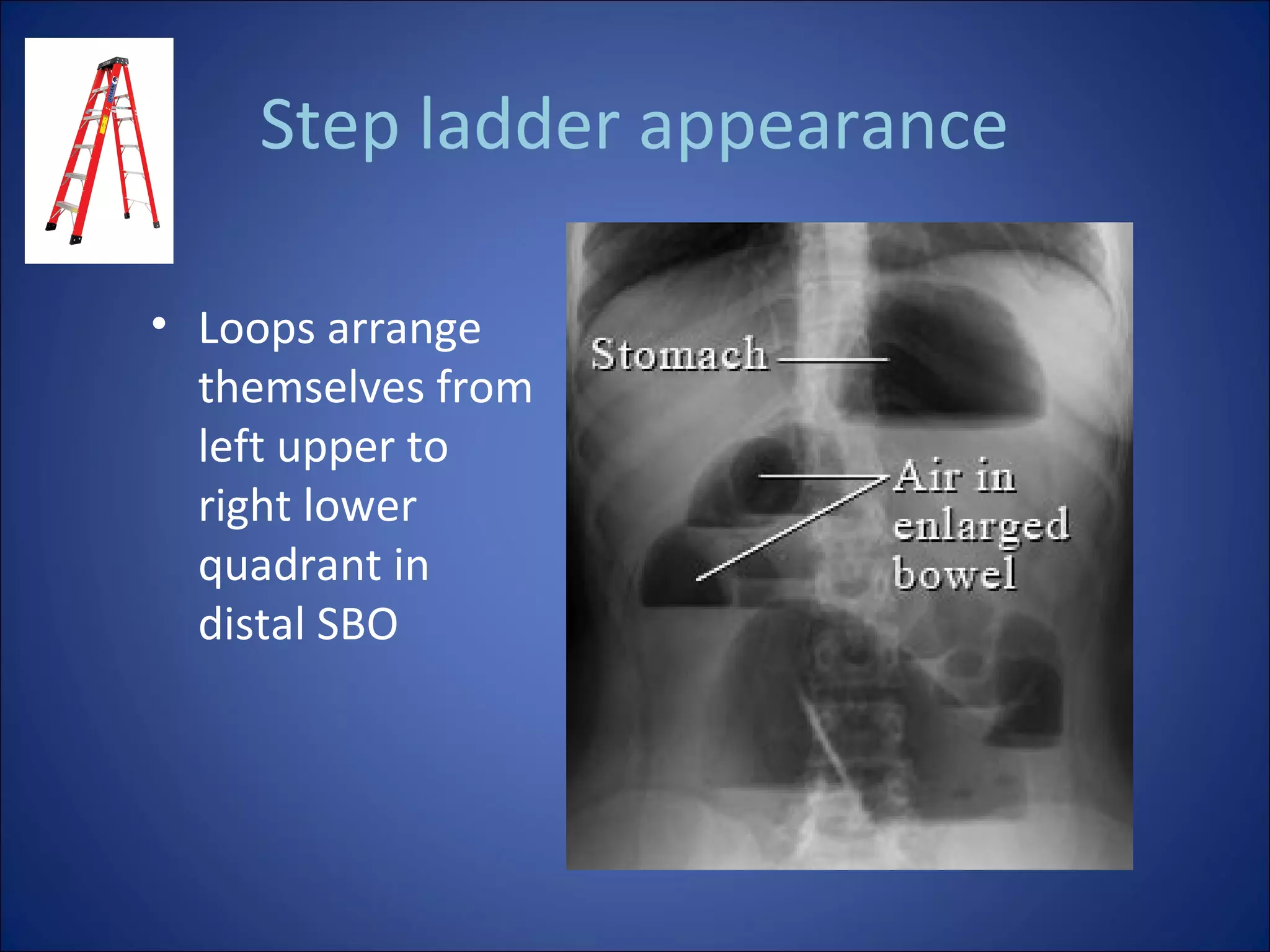
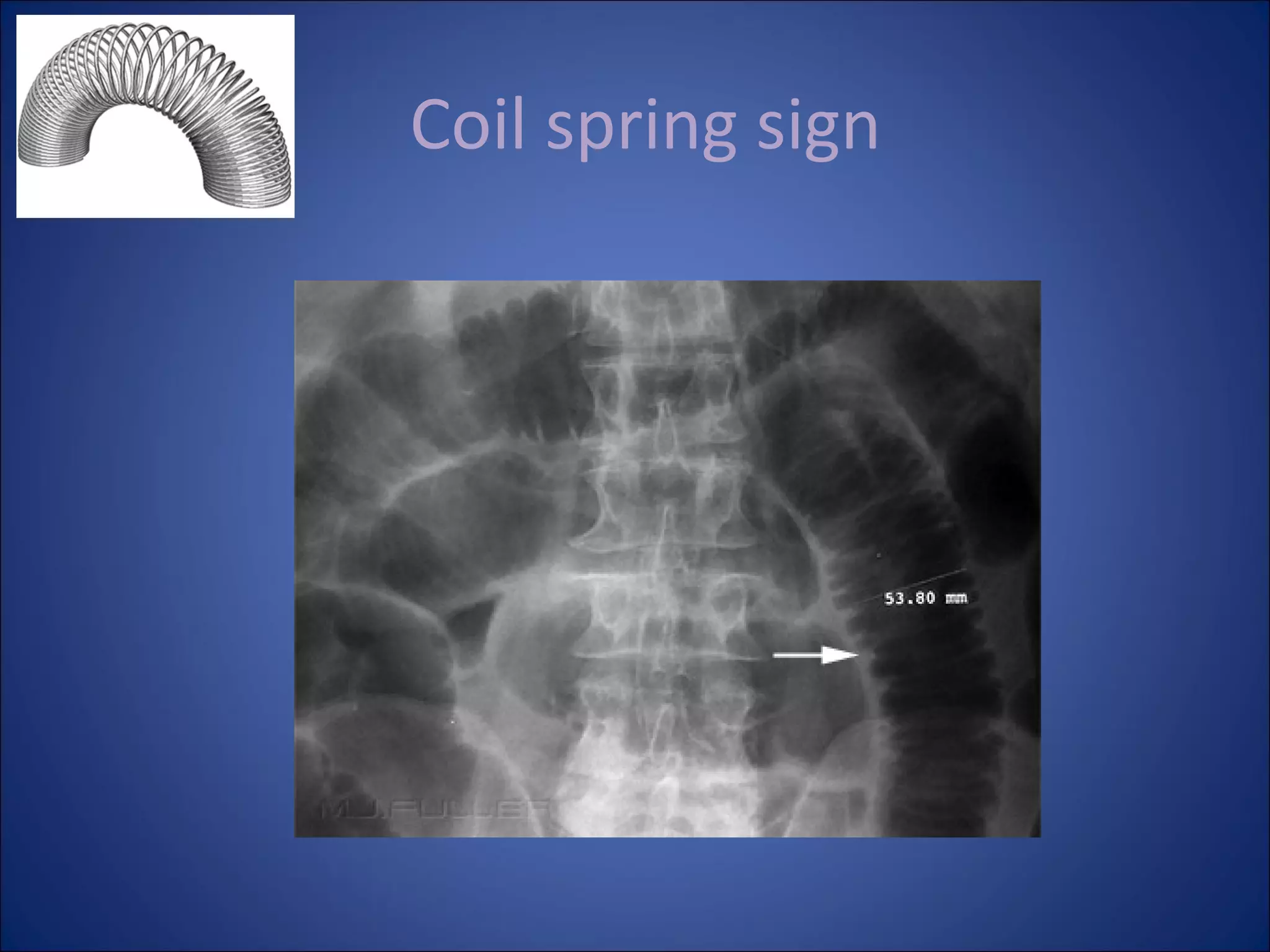
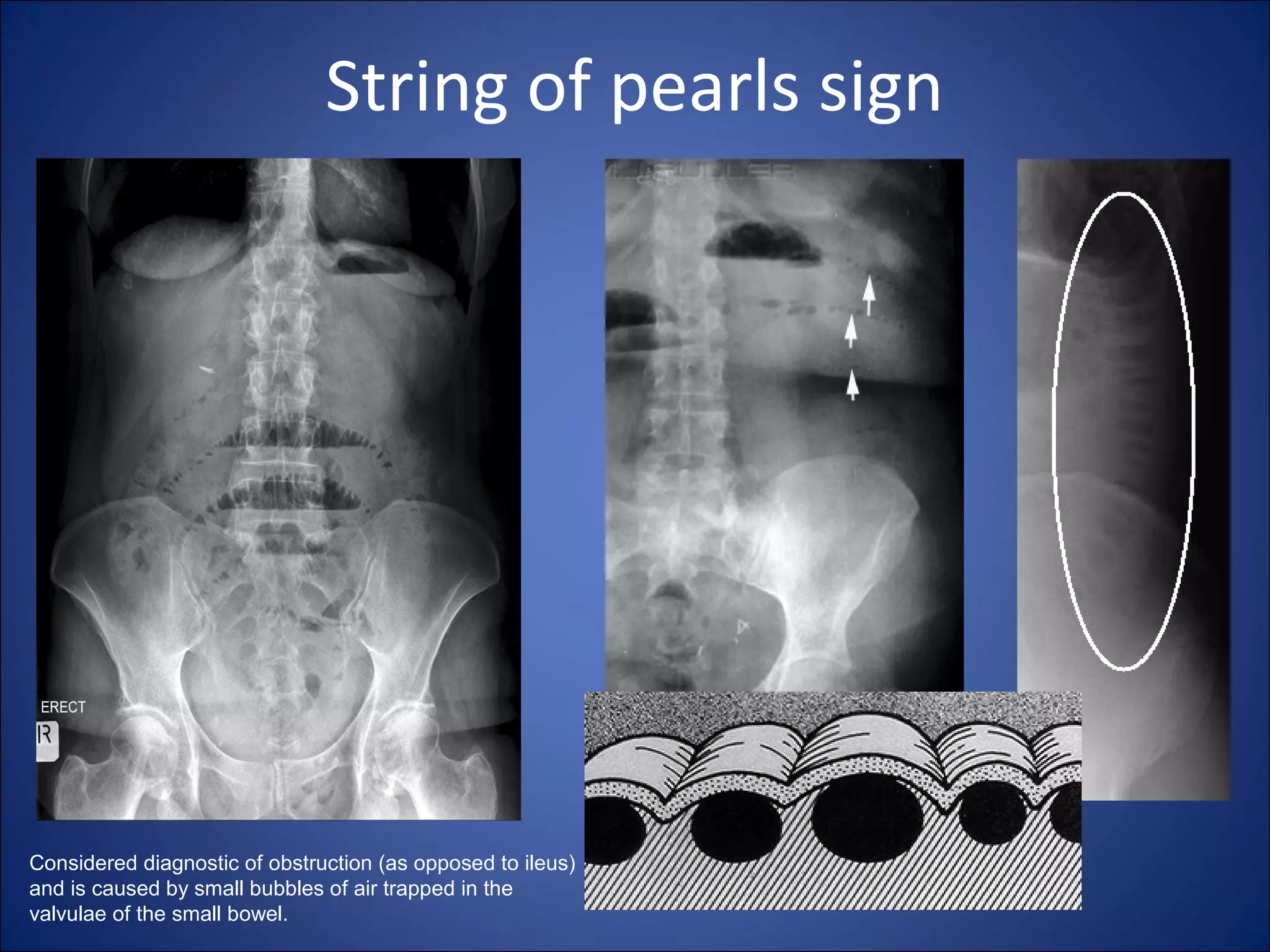


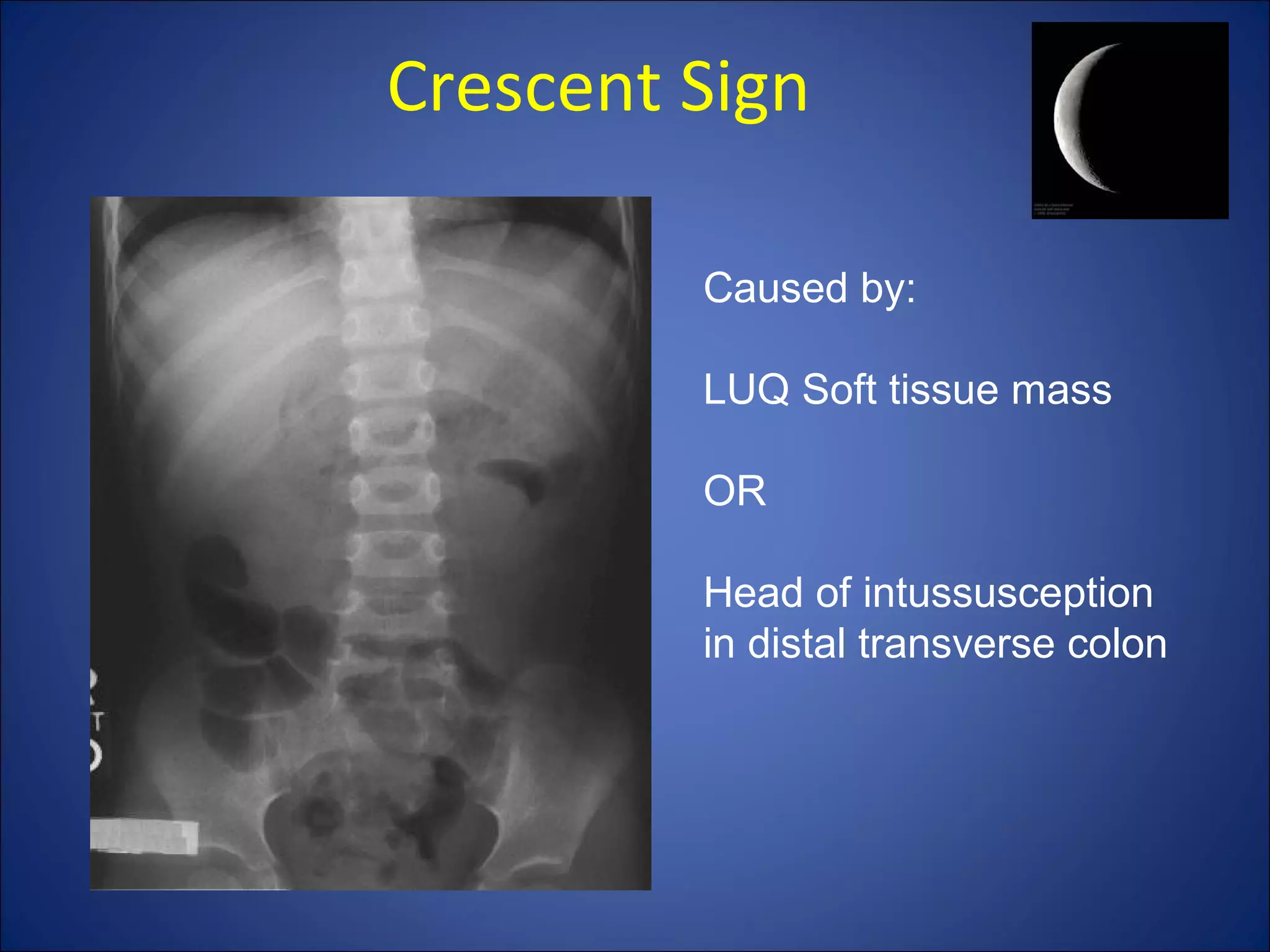
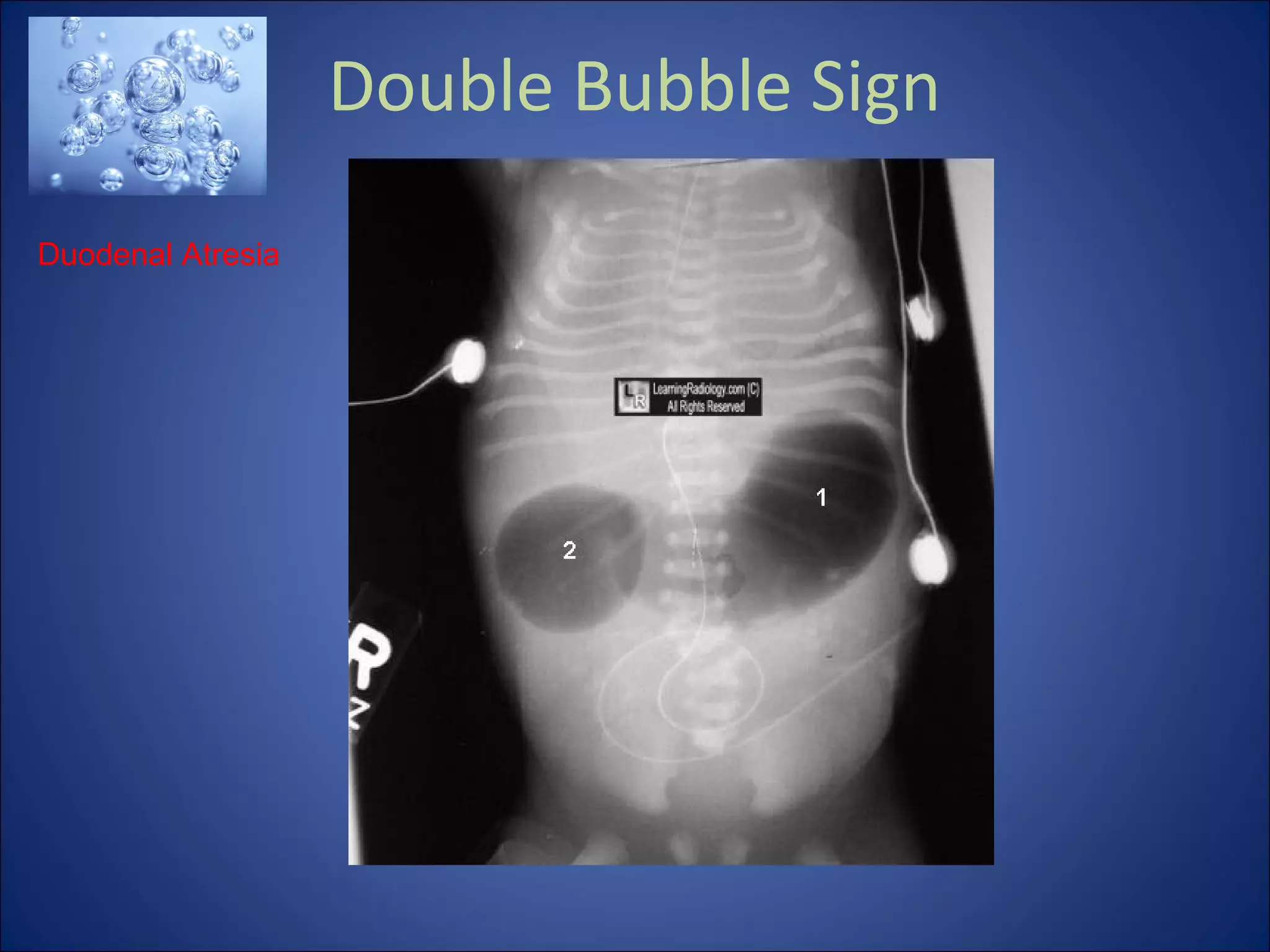

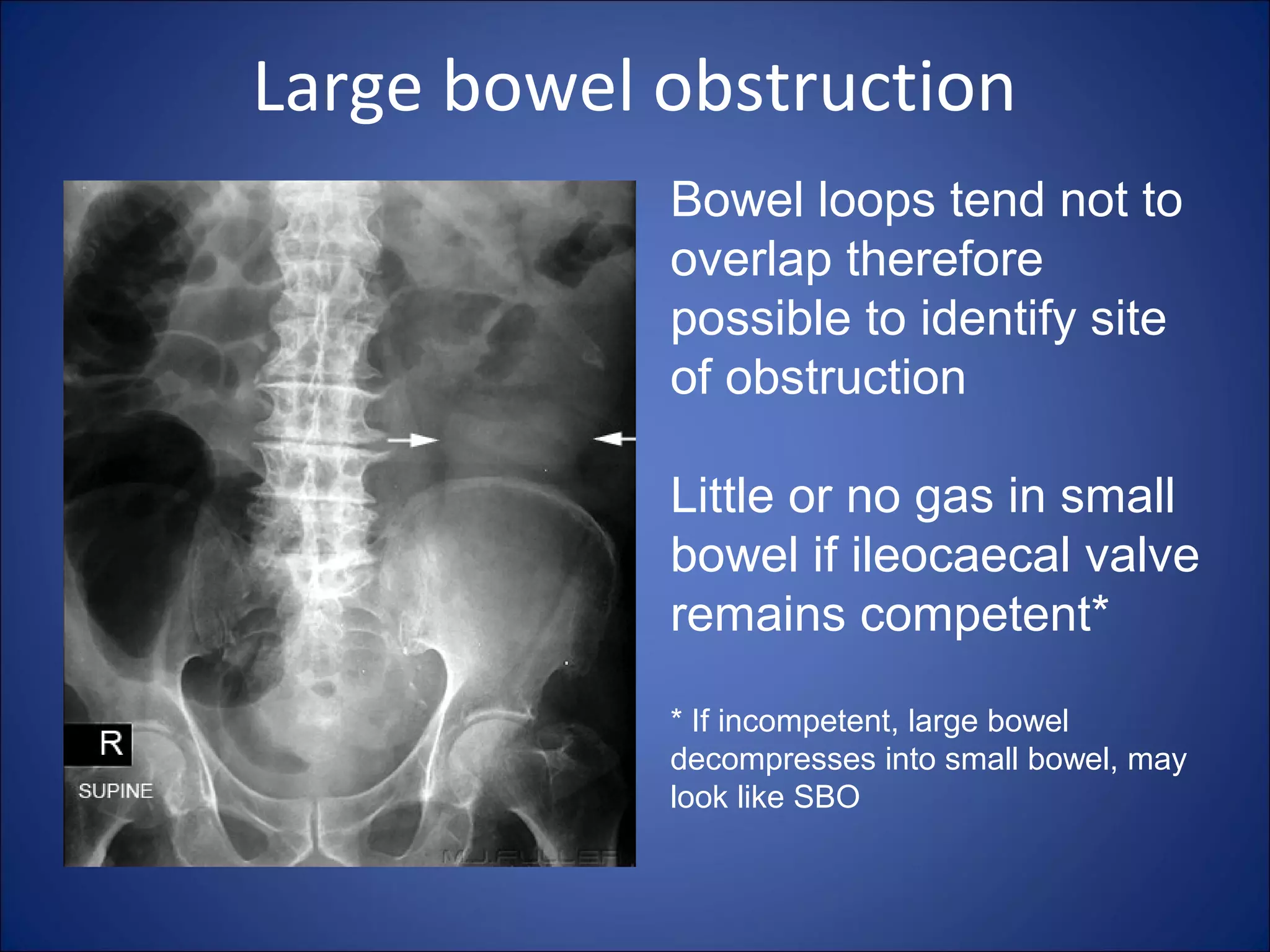

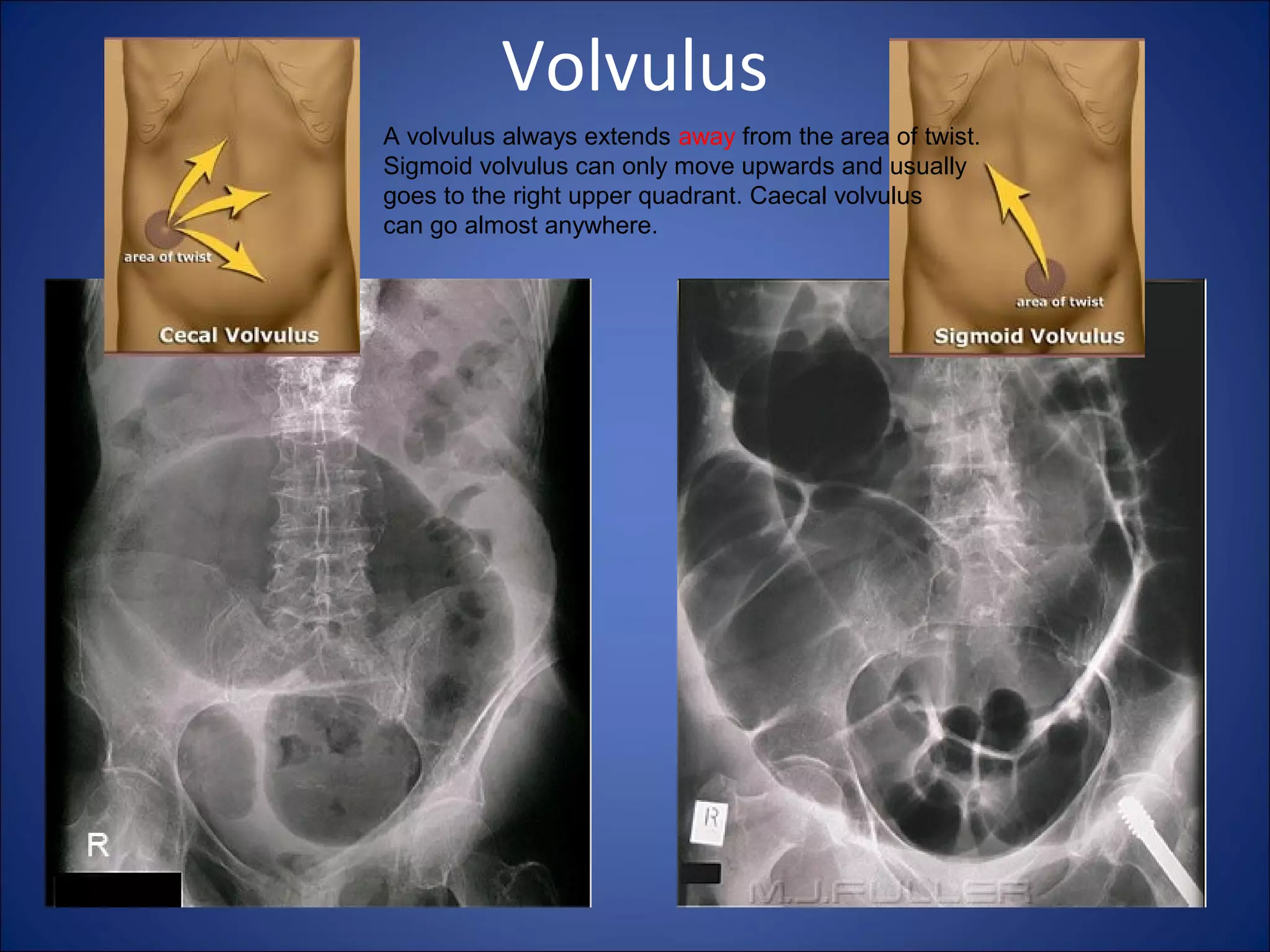






































This document provides an overview of normal and abnormal findings on abdominal x-rays. It describes the normal bowel gas pattern and anatomy seen on x-rays. Key signs of abdominal pathology are outlined, including localized ileus, mechanical small bowel obstruction, mechanical large bowel obstruction, and extraluminal air. Specific radiographic findings that help identify conditions like volvulus, hernia and malignancy are also reviewed. The document emphasizes the diagnostic value of obtaining multi-view x-rays to accurately evaluate abdominal abnormalities.























































































