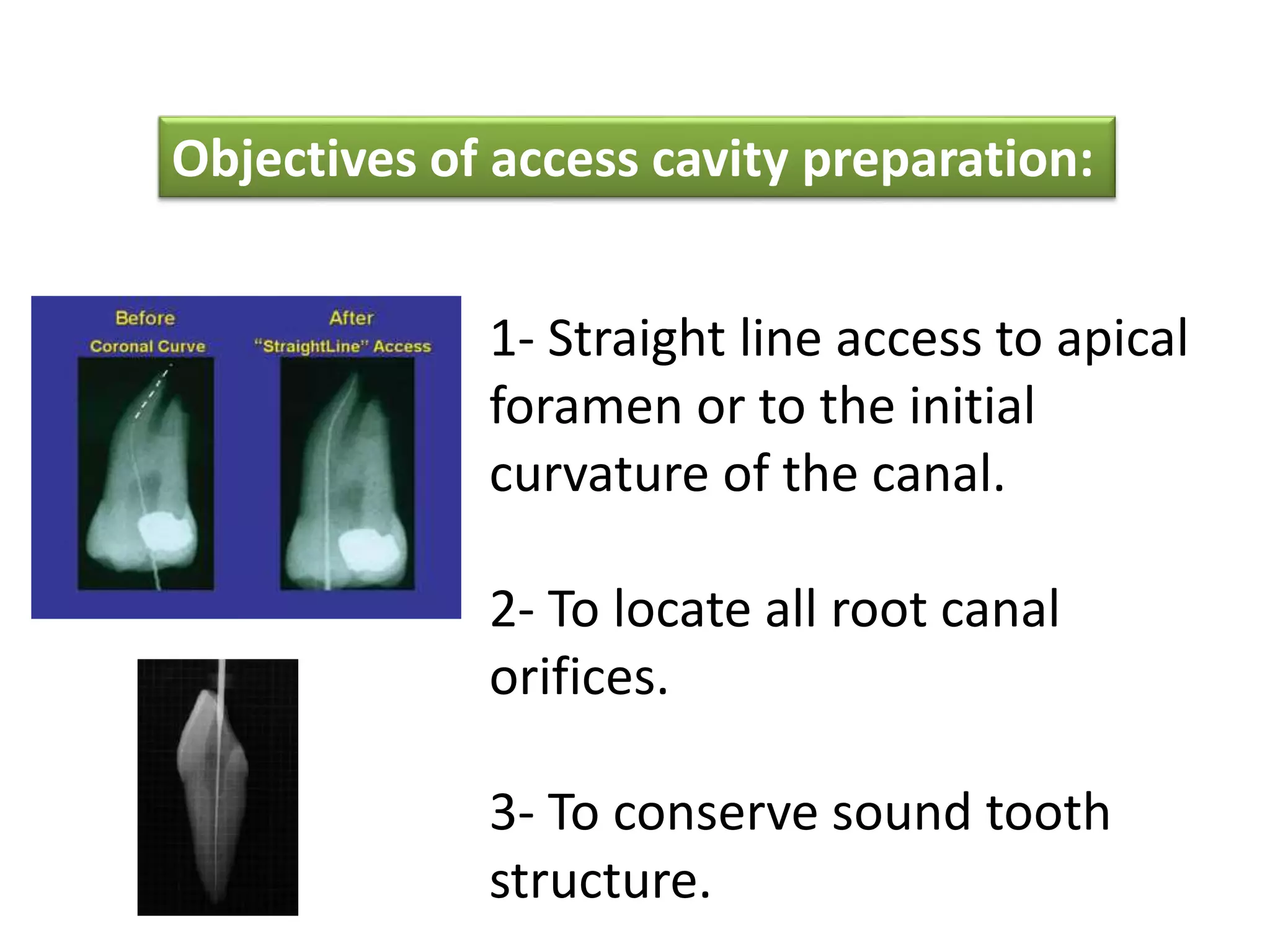
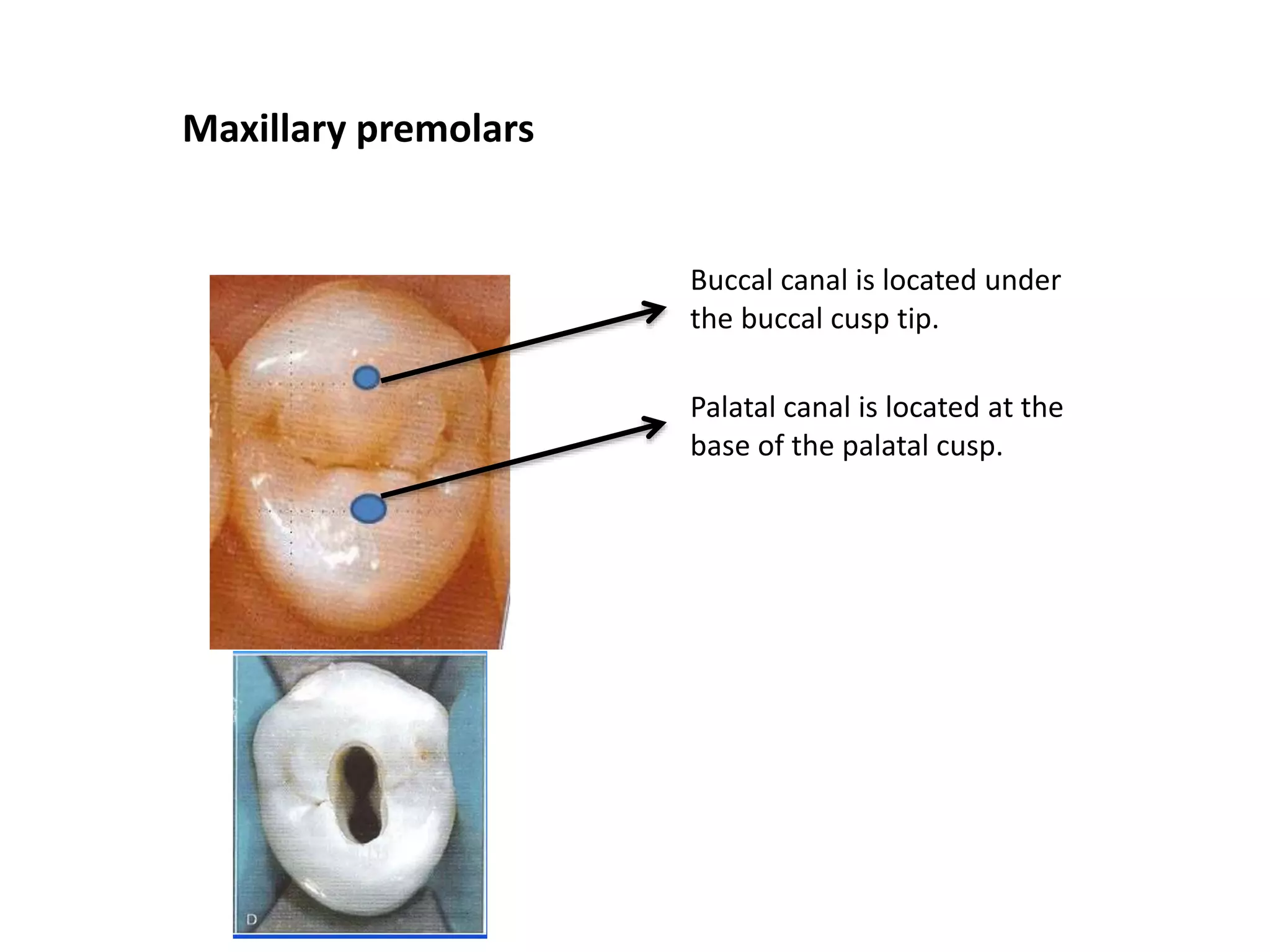
1. Access cavity preparation is the first and most important phase of root canal treatment, with the goals of achieving straight line access to the apical foramen, locating all root canal orifices, and conserving sound tooth structure.
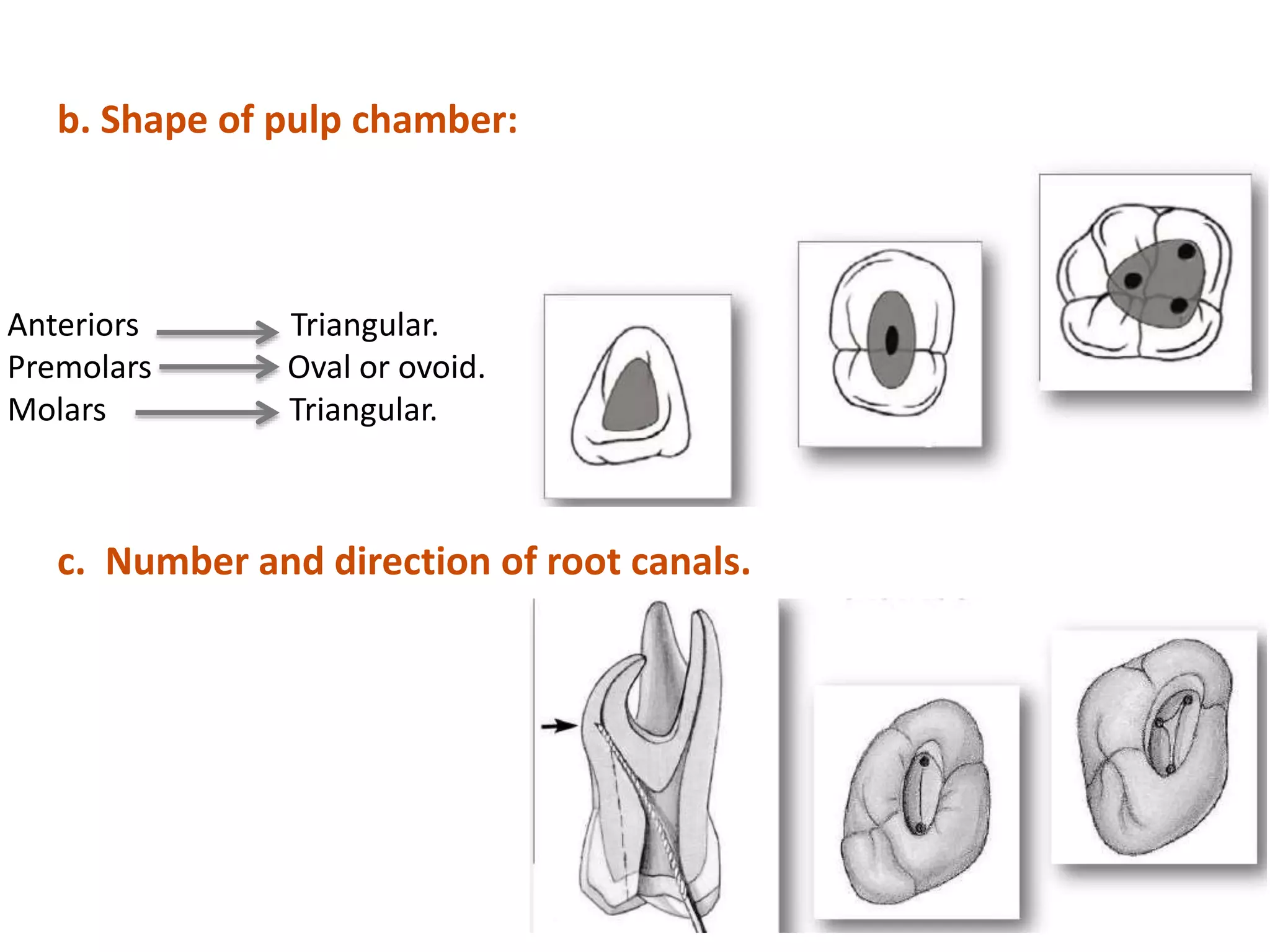
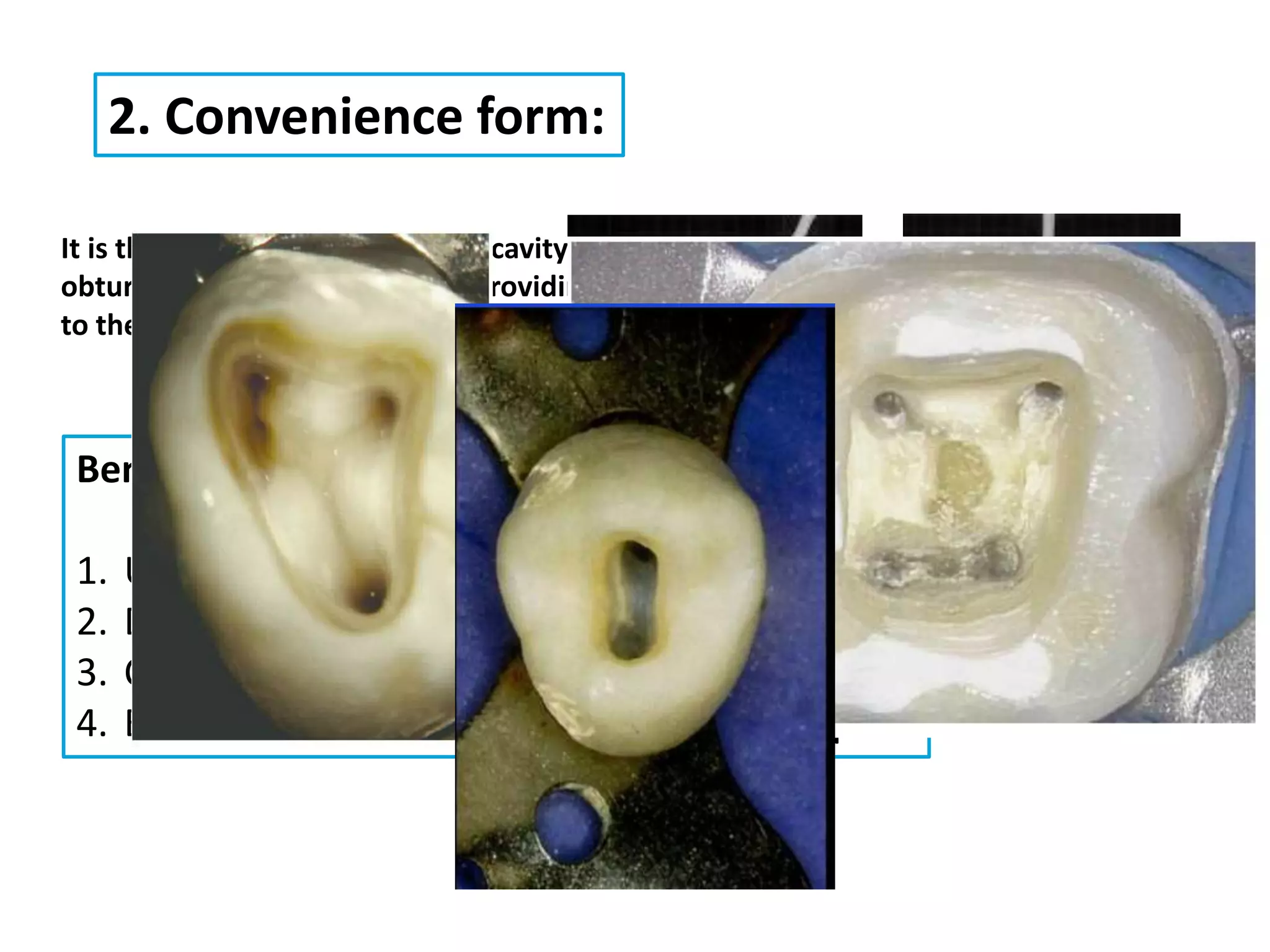
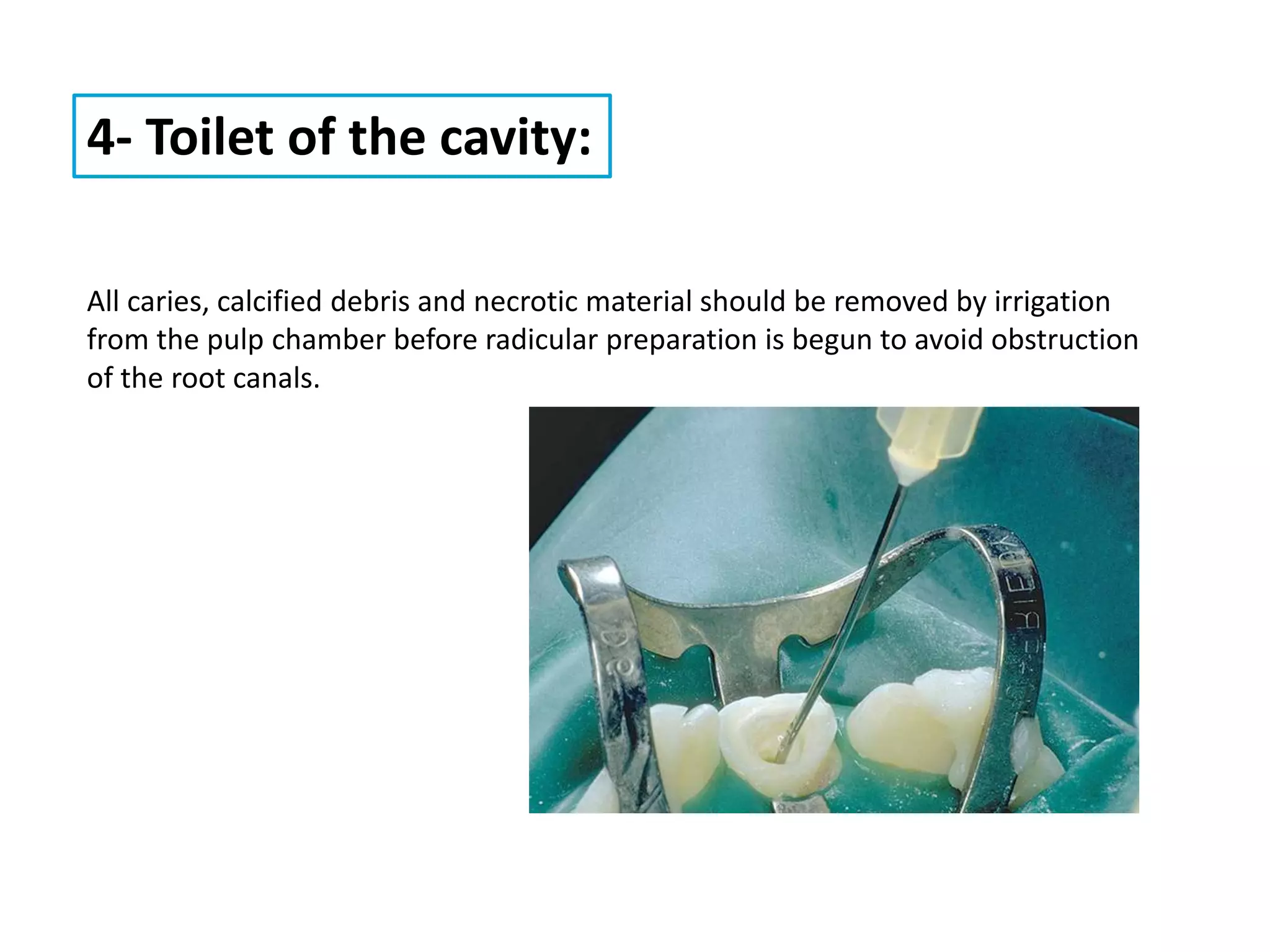
2. The principles of access cavity preparation include establishing an outline form based on pulp chamber size and shape and the number/direction of root canals, providing a convenience form for improved visibility and instrumentation, and removing caries/defective restorations and debris from the pulp chamber.
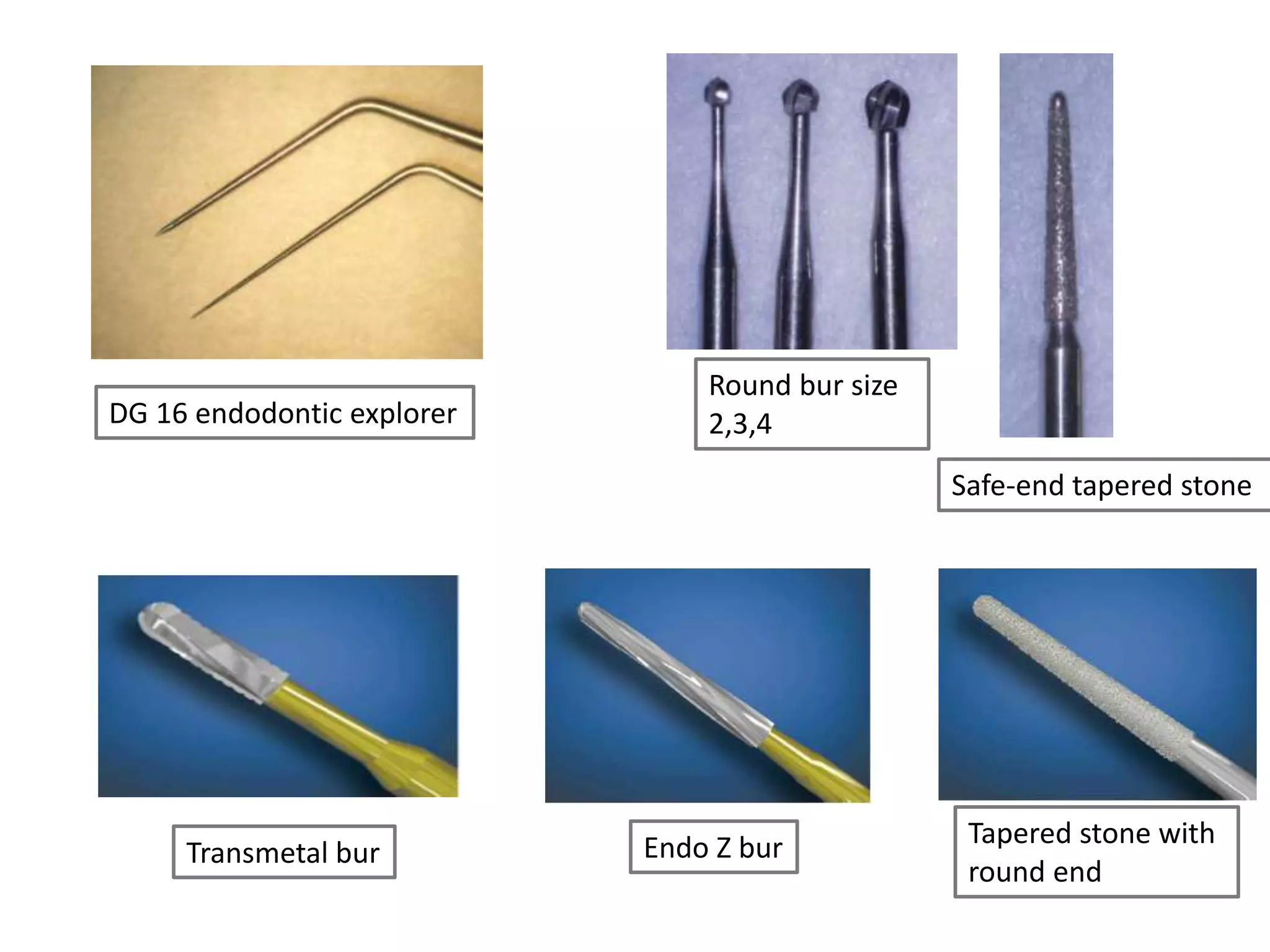
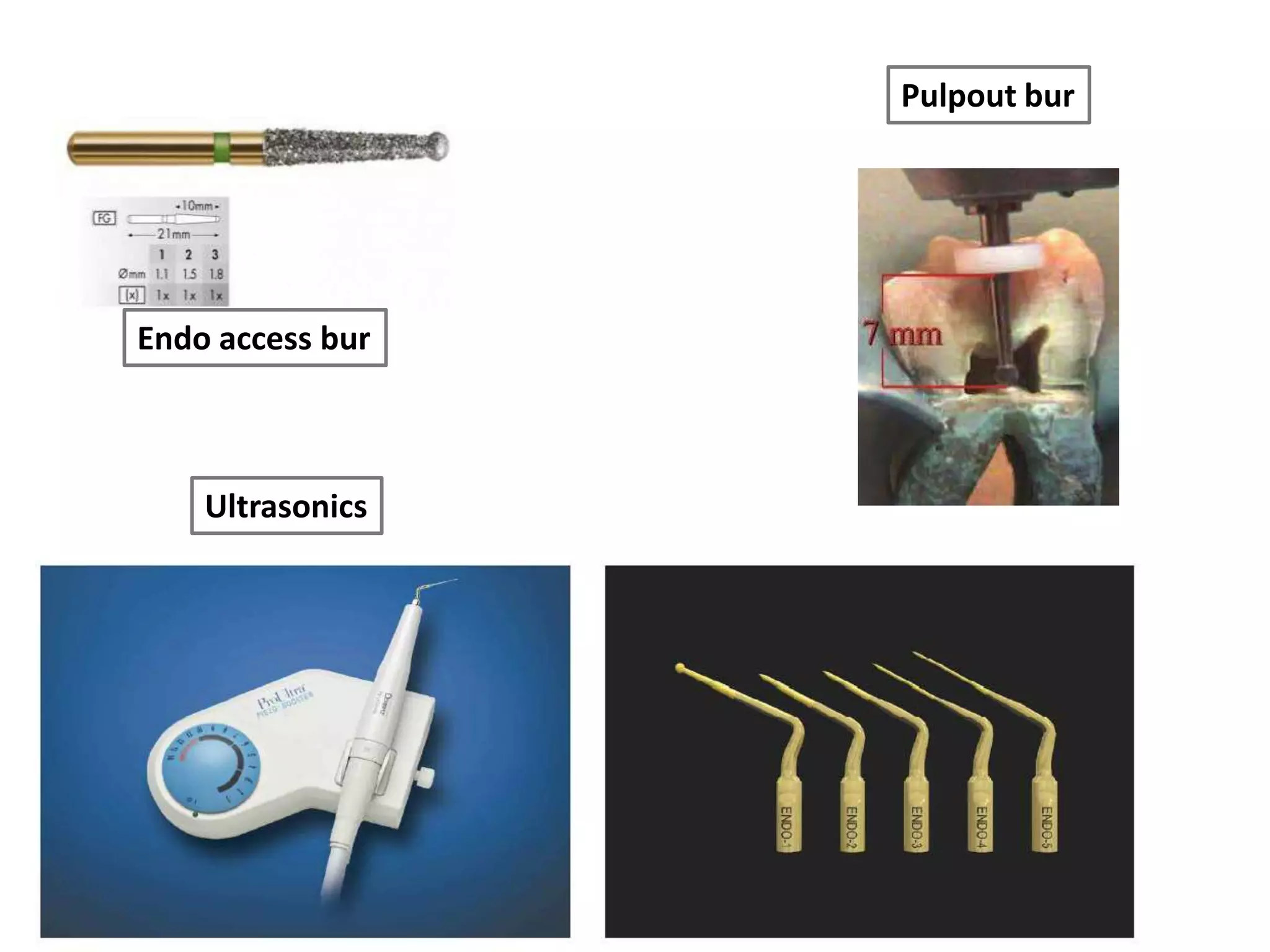
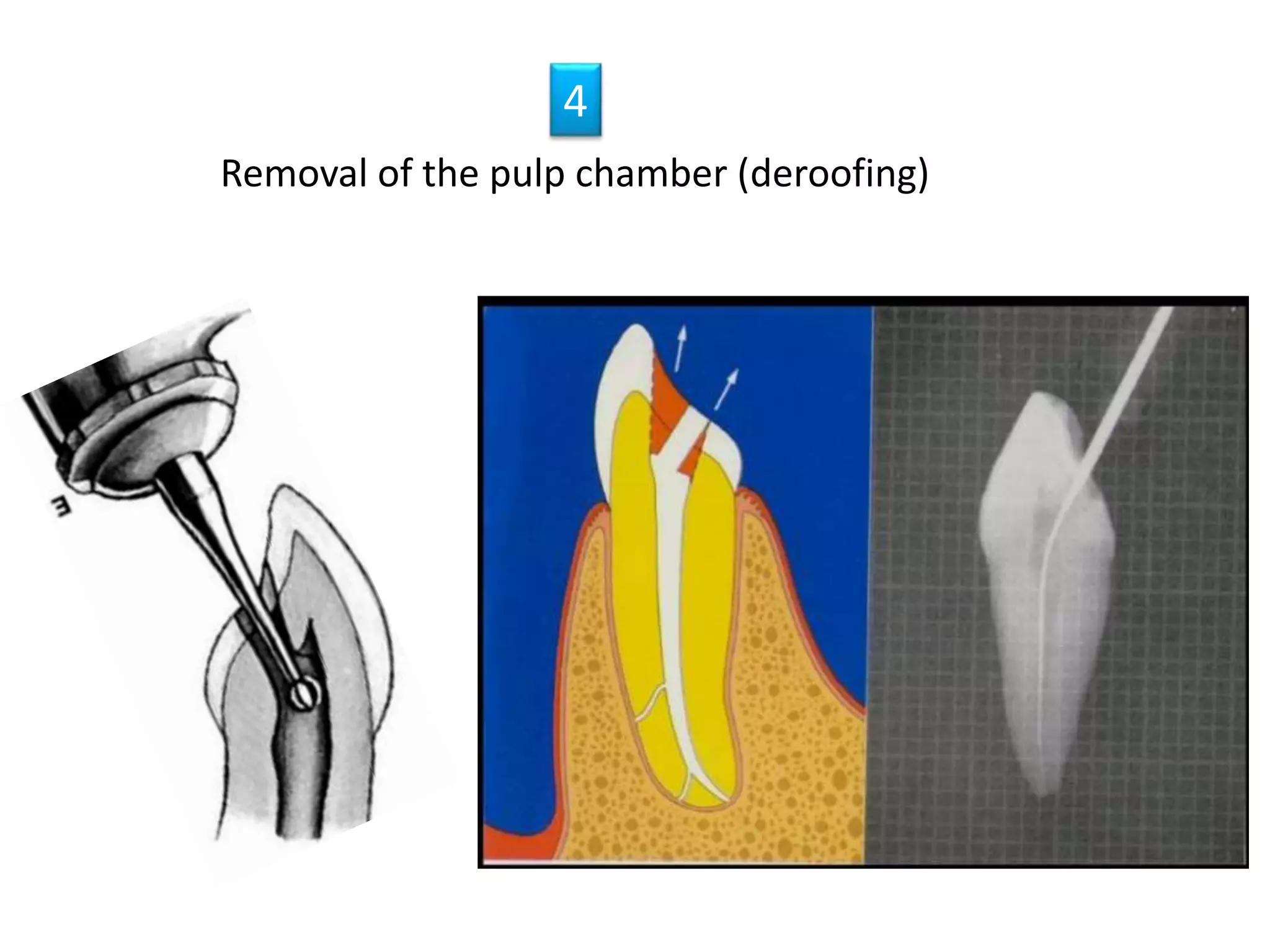
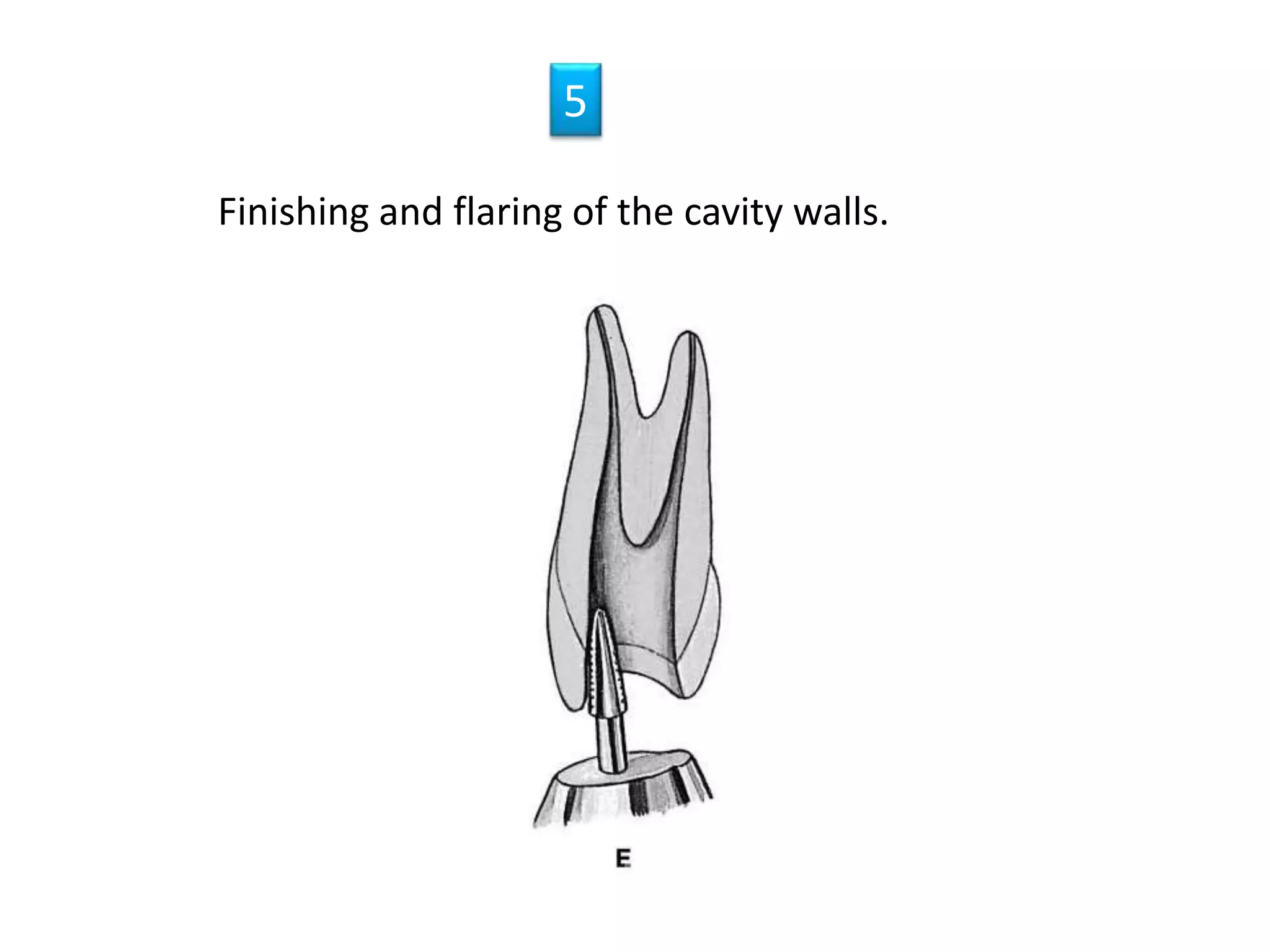
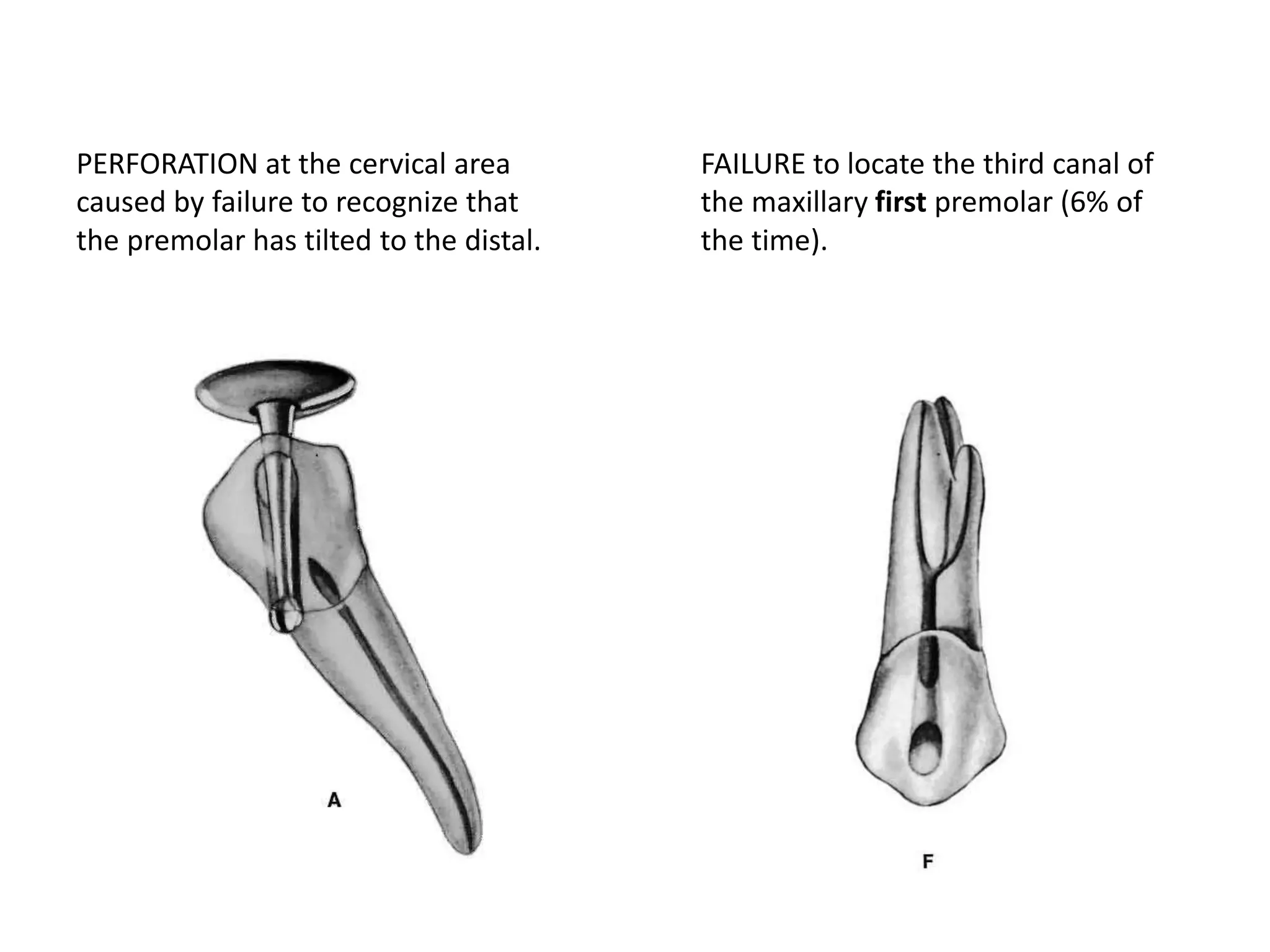
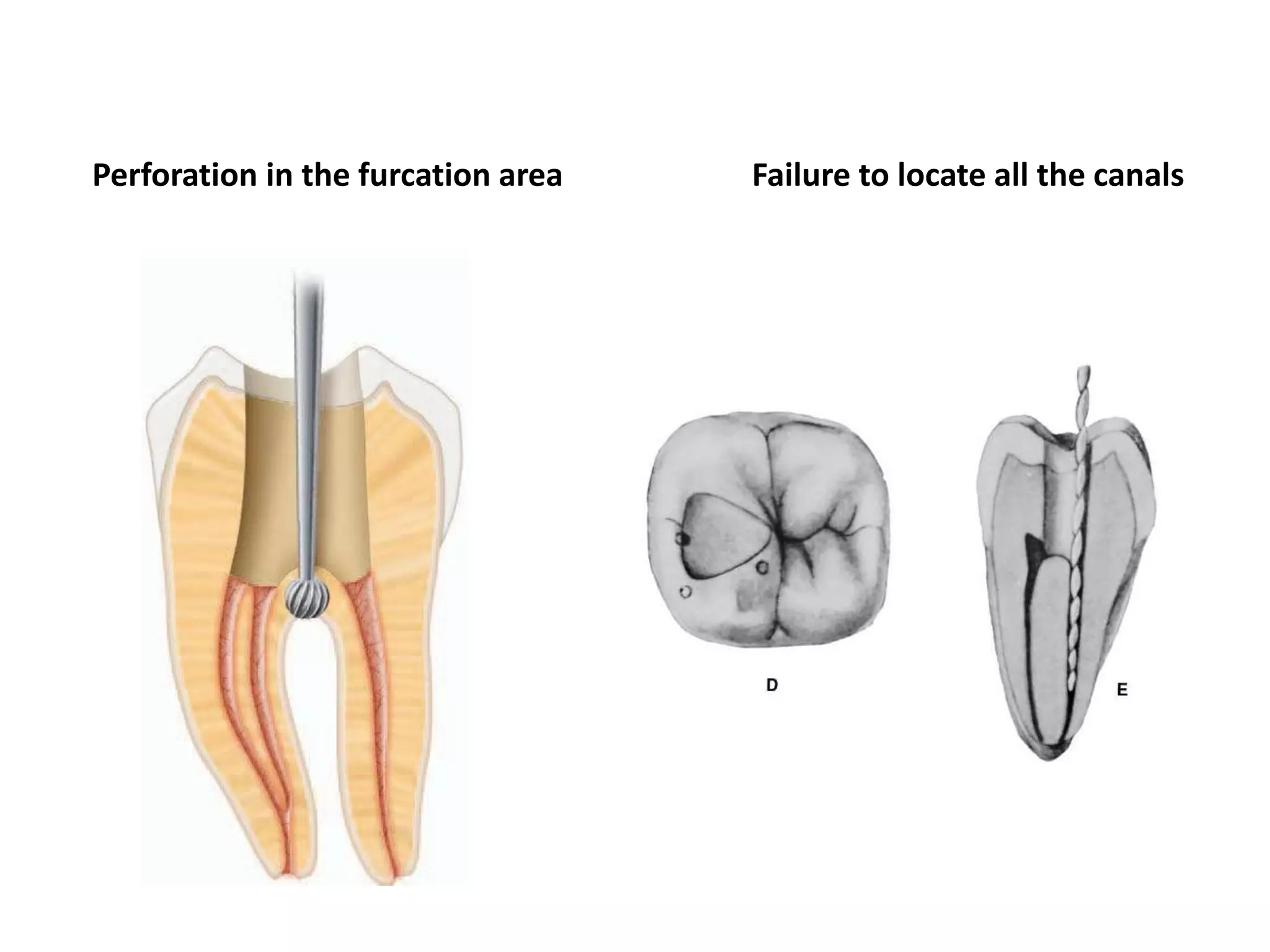
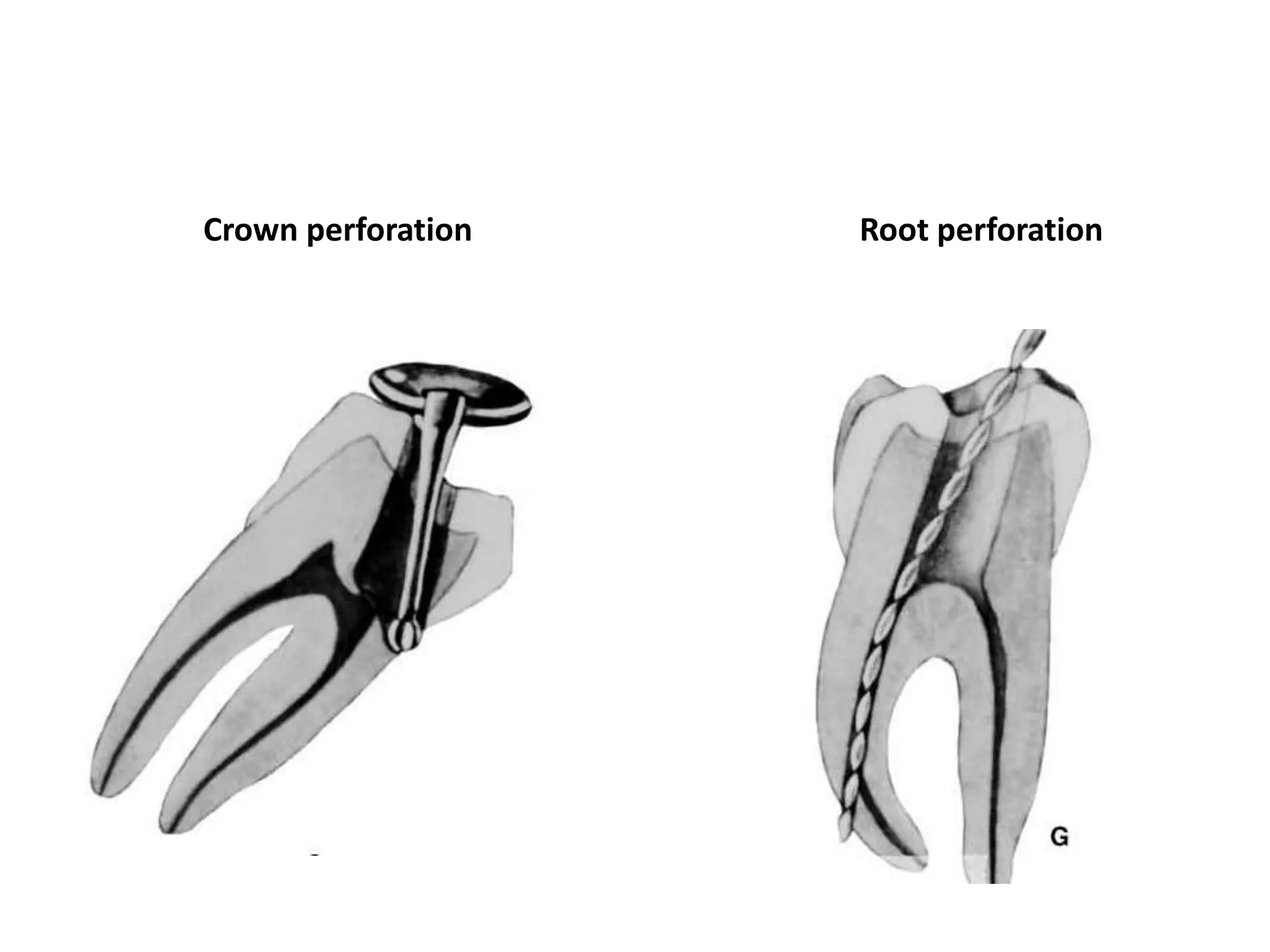
3. Key steps in access cavity preparation depend on the specific tooth but involve using burs and instruments to locate and prepare access to all root canal orifices while avoiding errors like



























































![Tools of dental_public_health[1]](https://cdn.slidesharecdn.com/ss_thumbnails/toolsofdentalpublichealth1-151108134342-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)