Downloaded 301 times
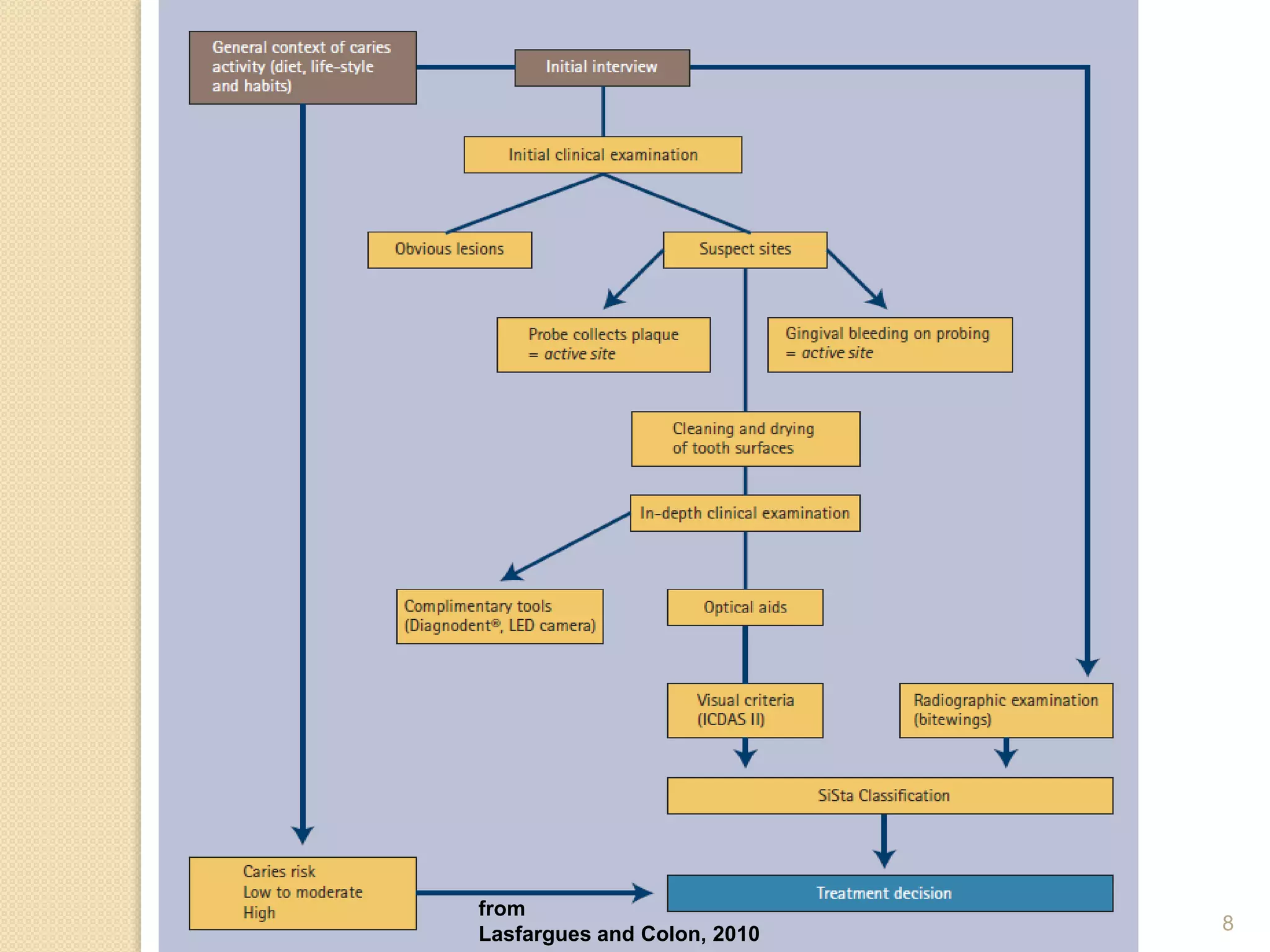
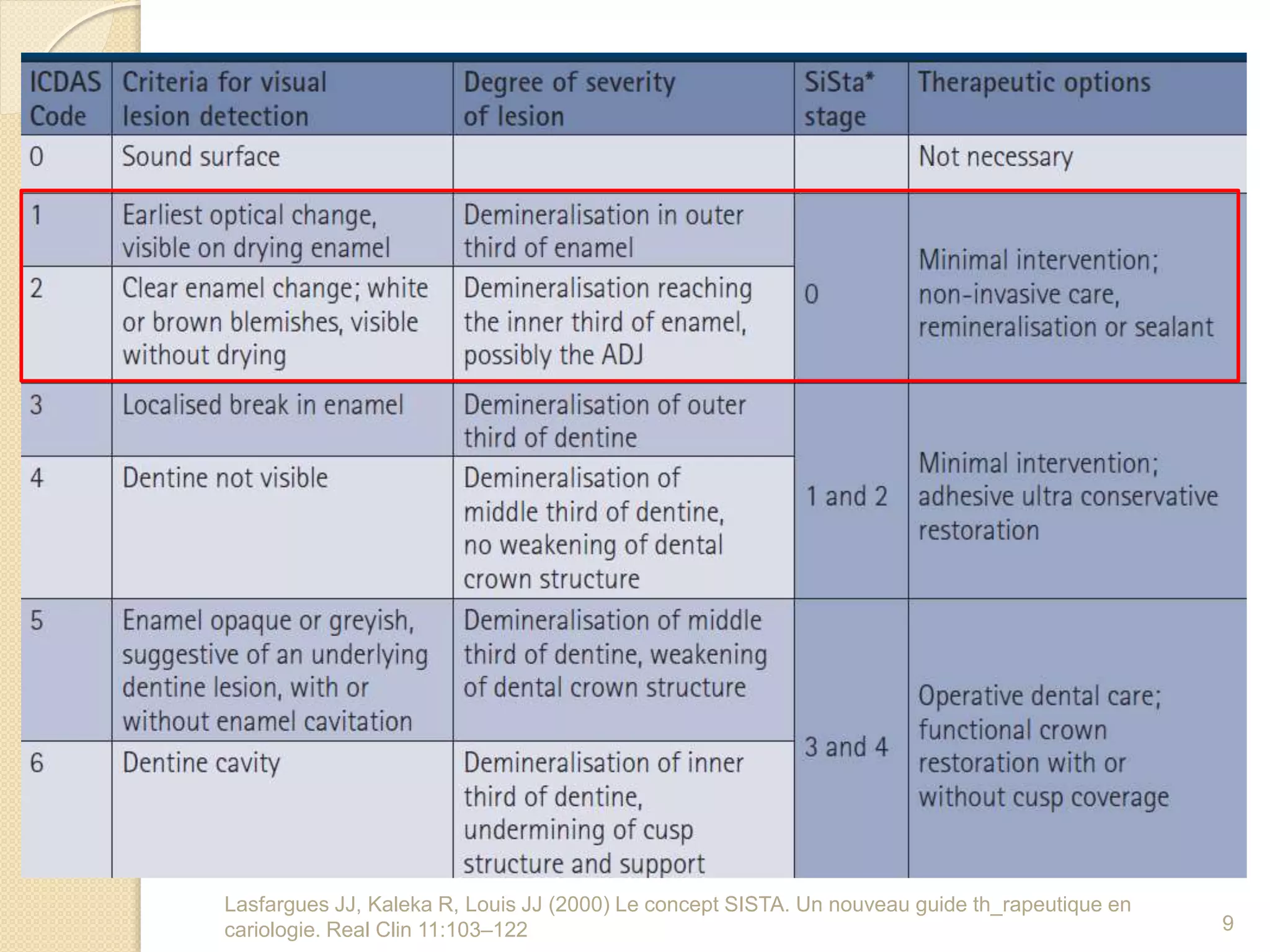
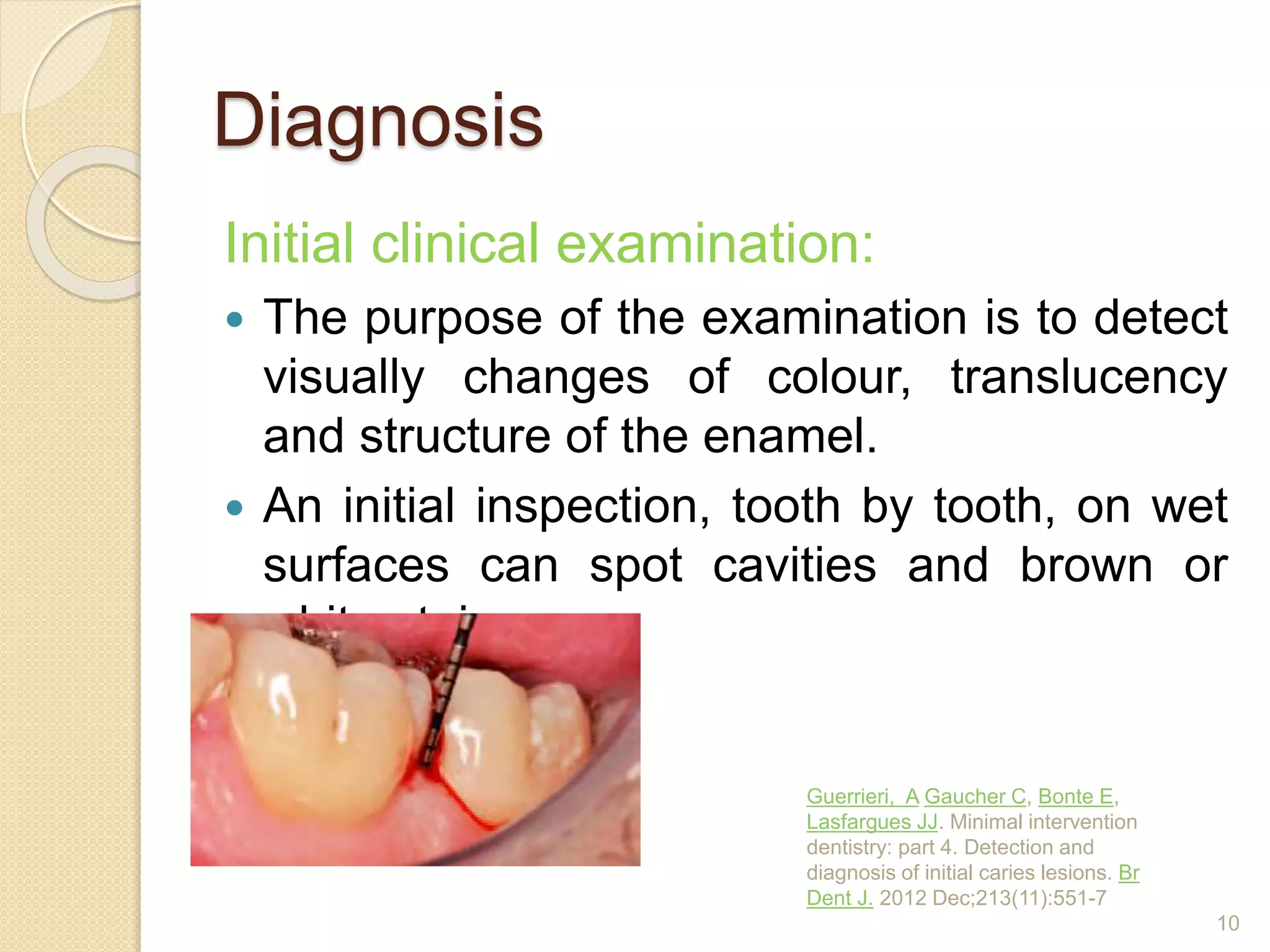

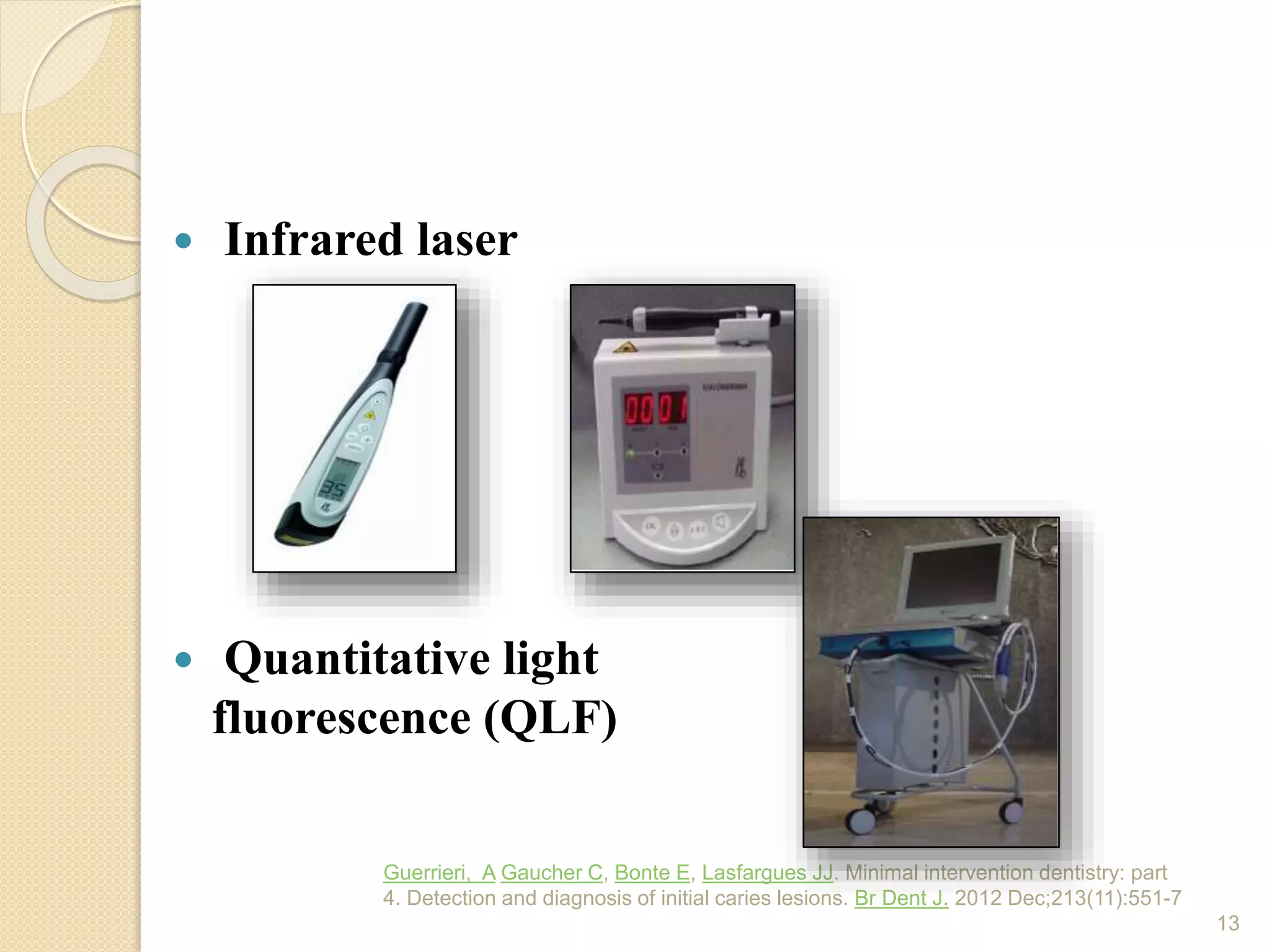
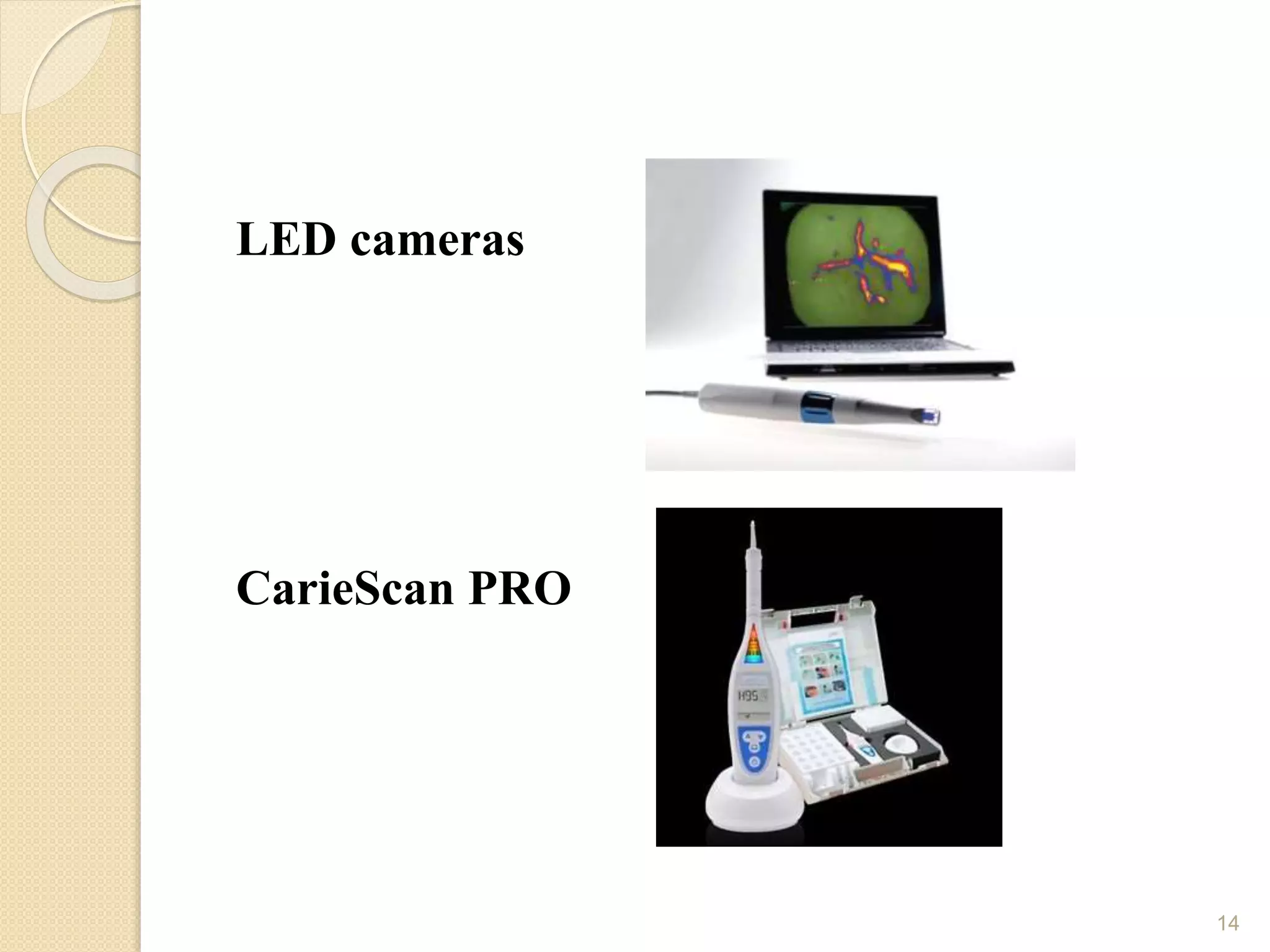
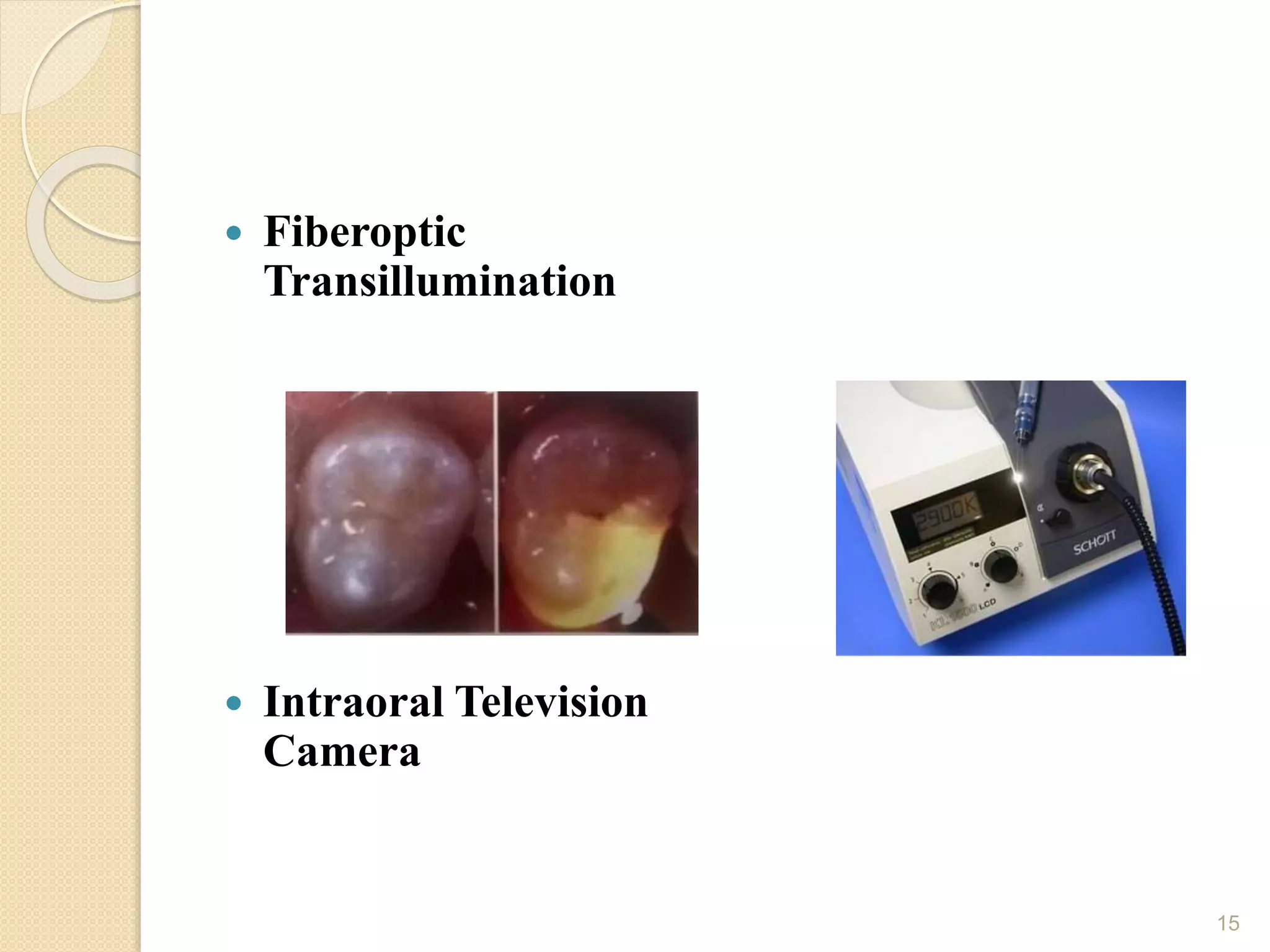
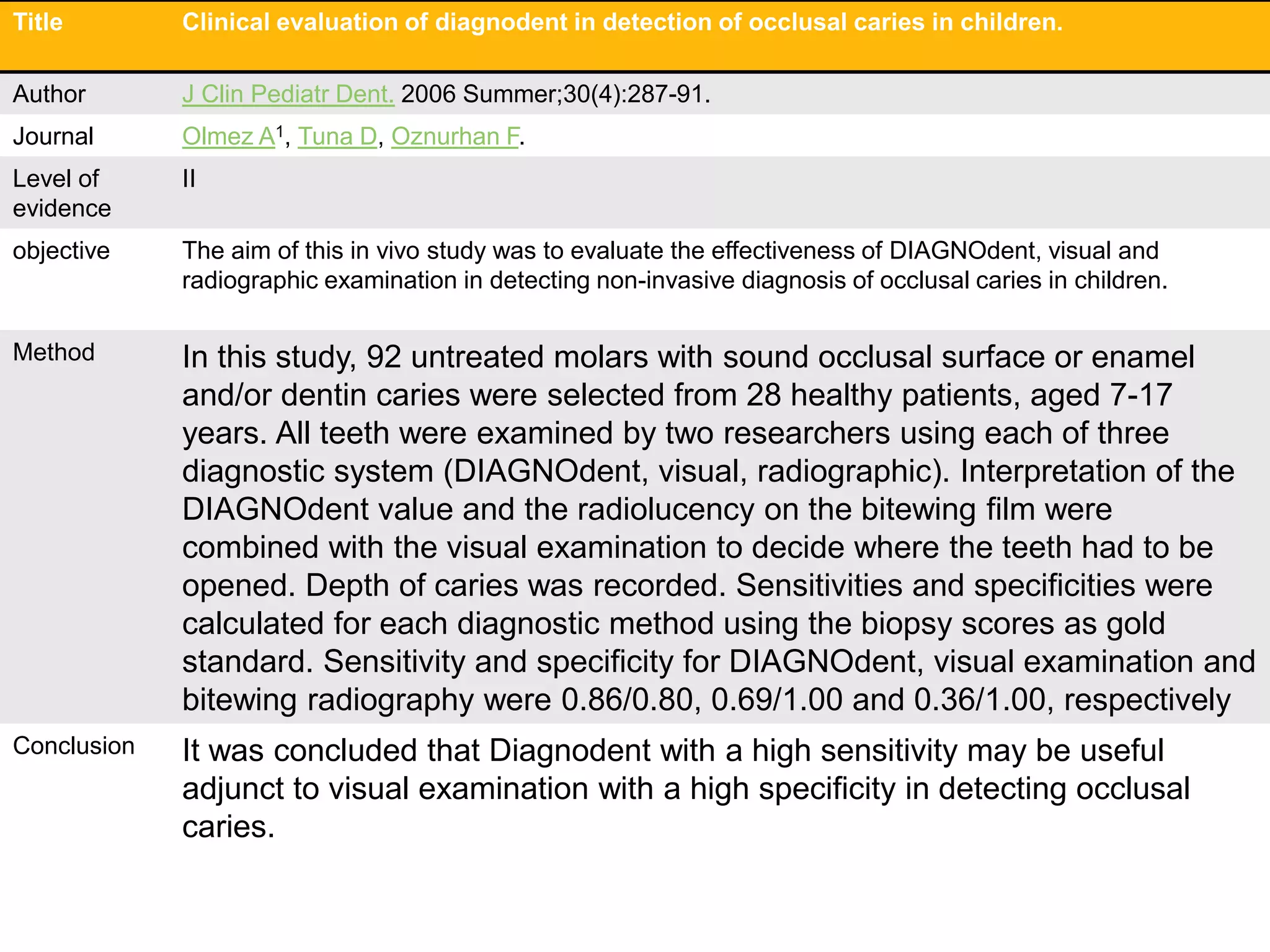
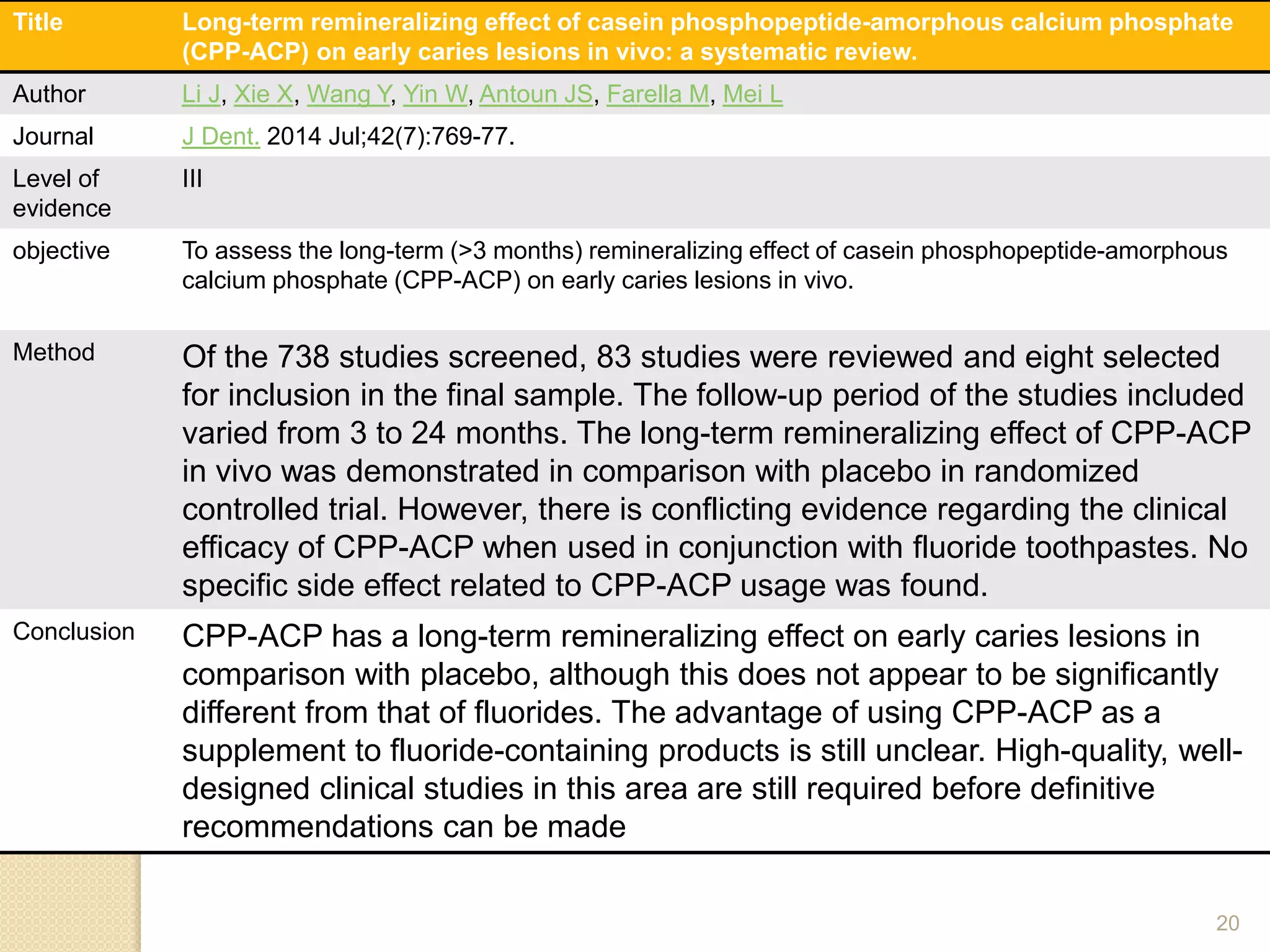


The document discusses incipient carious lesions, also known as white spot lesions. It defines incipient caries as the earliest sign of demineralization appearing as a chalky white spot. Diagnosis involves visual examination and aids like radiographs, fluorescence systems, and LED cameras to detect early mineral changes. Management focuses on remineralization through fluoride and remineralizing agents like CPP-ACP to control demineralization using non-operative procedures and potentially reverse early lesions.





































![[1][m] minimally invasive restorative dentistry](https://cdn.slidesharecdn.com/ss_thumbnails/1mminimallyinvasiverestorativedentistry-160422162403-thumbnail.jpg?width=640&height=640&fit=bounds)



































