The document provides information on common poisonings. It notes that in the UK there are approximately 300,000 cases of poisoning annually, with 100,000 hospital admissions and 3,500-4,000 deaths. Poisonings can involve prescription drugs, over-the-counter drugs, alcohol, and illicit drugs. Management of poisonings primarily involves supportive care, such as maintaining airway, breathing, circulation, and treating complications like seizures or abnormal vital signs. Specific antidotes exist for only a minority of poisonings.
![ASPIRIN
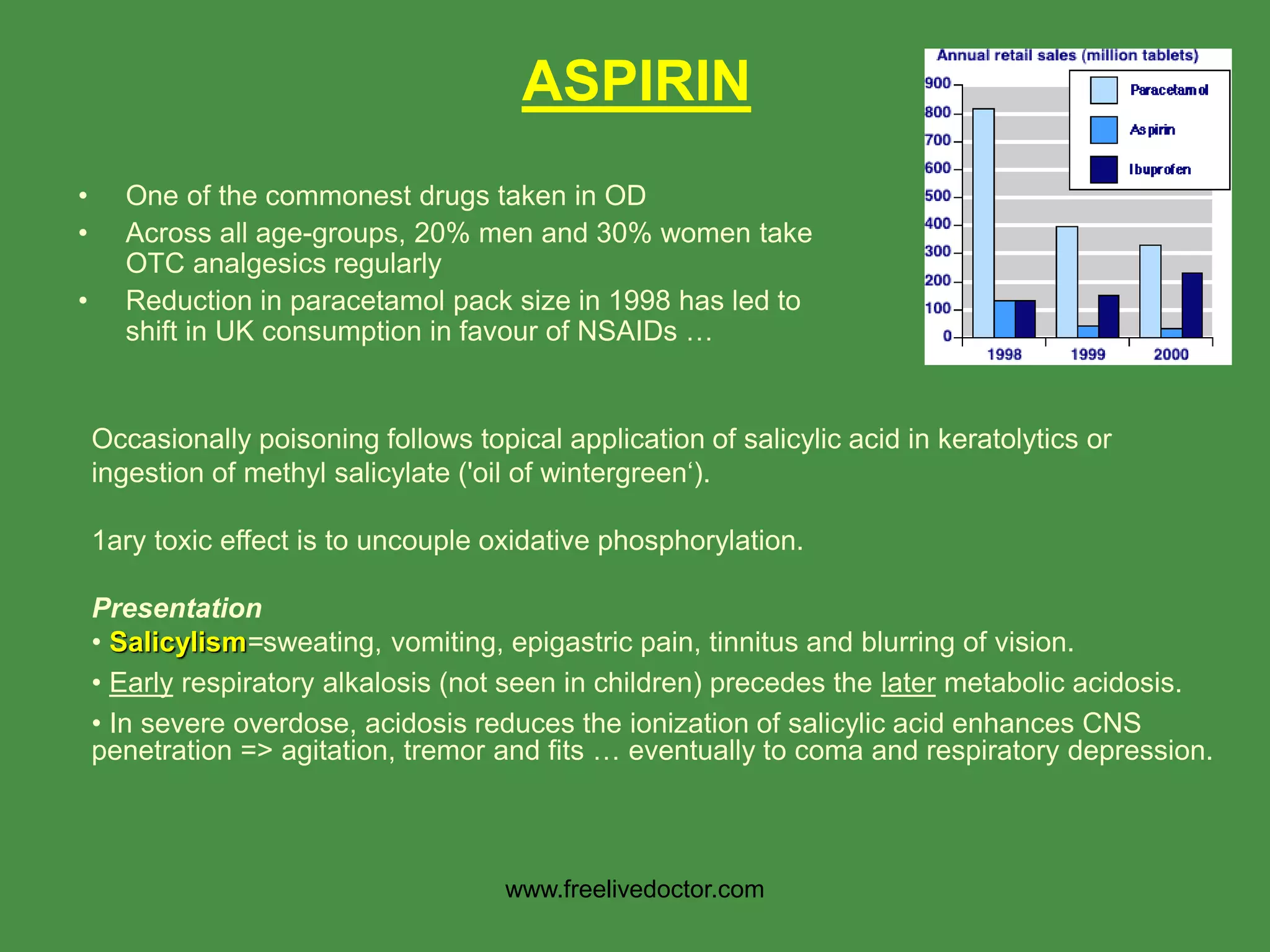
Complications
• Electrolyte Disturbance universal
hypokalaemia and deranged Na+ (high > low)
glucose (hyper > hypo)
• Pulmonary oedema (often non-cardiogenic) & acute renal failure.
• Hypoprothrombinaemia is very rare.
• Significant GI bleeds are surprisingly infrequent.
Management - therapeutic [salicylate] is <300mg/l (2.2 mmol/l)
Mild/moderate salicylism requires only rehydration + KCl supplements.
Marked salicylism or levels > 750mg/l need specific elimination therapy:
(1) Oral activated charcoal (50g 4 hourly)
(2) Forced alkaline diuresis NO LONGER RECOMMENDED - it is no more effective
than simple alkalinisation (eg 1 L 1.26% NaHCO3 over 2 hrs and repeated to keep the
urinary pH > 7.5).
(3) Haemodialysis is required for any of the following: level >1000mg/1 (7.25 mmol/l);
persistent/progressive acidosis; deteriorating level of consciousness.
www.freelivedoctor.com](https://image.slidesharecdn.com/commonpoisonings-100420022313-phpapp01/75/Common-poisonings-5-2048.jpg)
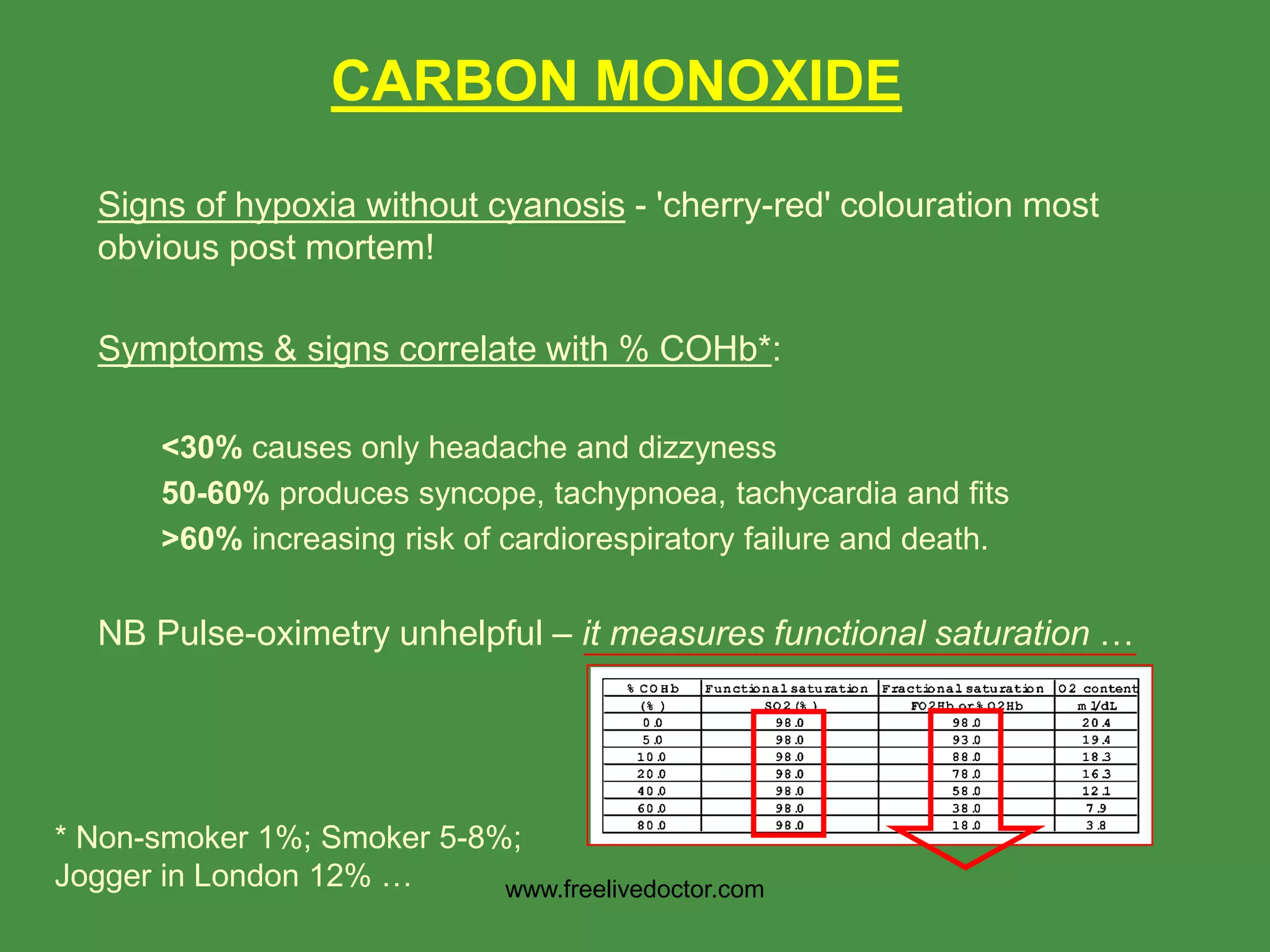
![CARBON MONOXIDE
Management
• Check ABG - PaO2 may be normal but metabolic acidosis indicates
severe poisoning.
• Give O2 by mask unless comatose then IPPV with FiO2 =1 (t1/2
COHb 320 mins on room air vs 80 mins at 100%)*. [Also consider if
severely acidotic or evidence of myocardial ischaemia.]
• Control fits with IV diazepam.
Hyperbaric 02 will shorten the washout of
COHb further (half-life of 25 mins at 2
atmospheres), but access and transfer
times to a hyperbaric chamber may make
this impractical. Recent trial suggest may be
worthwhile (cognitive sequelae at 6/52 were
reduced from 35/76 to 19/76 by this Rx ….
NEJM 2002;347:1057
www.freelivedoctor.com](https://image.slidesharecdn.com/commonpoisonings-100420022313-phpapp01/75/Common-poisonings-14-2048.jpg)
![Presentation – following typical of amphetamines but not
features of usual recreational doses of E
• Sympathomimetic effects - mydriasis, BP, HR, skin pallor.
• Central effects - hyperexcitability, talkativeness and agitation.
• [Paranoid features may be obvious especially in chronic users
– not applicable to E].
Complications
• A 'heat-stroke' like syndrome: rhabdomyolysis, hyperpyrexia
(>42 C), DIC and acute renal failure. It carries a poor
prognosis (see cocaine). ? PK problem ?? CYP2D6
metaboliser status important
• [Intracranial (and subarachnoid) haemorrhage (? 2ary to
hypertensive effect but can occur after single therapeutic
doses and vasospasm reported at angiography 'string-of-
beads' sign) – not applicable to E].
3,4-methylenedioxy-methamphetamine
(MDMA, Ecstasy)
www.freelivedoctor.com](https://image.slidesharecdn.com/commonpoisonings-100420022313-phpapp01/75/Common-poisonings-25-2048.jpg)