Downloaded 62 times








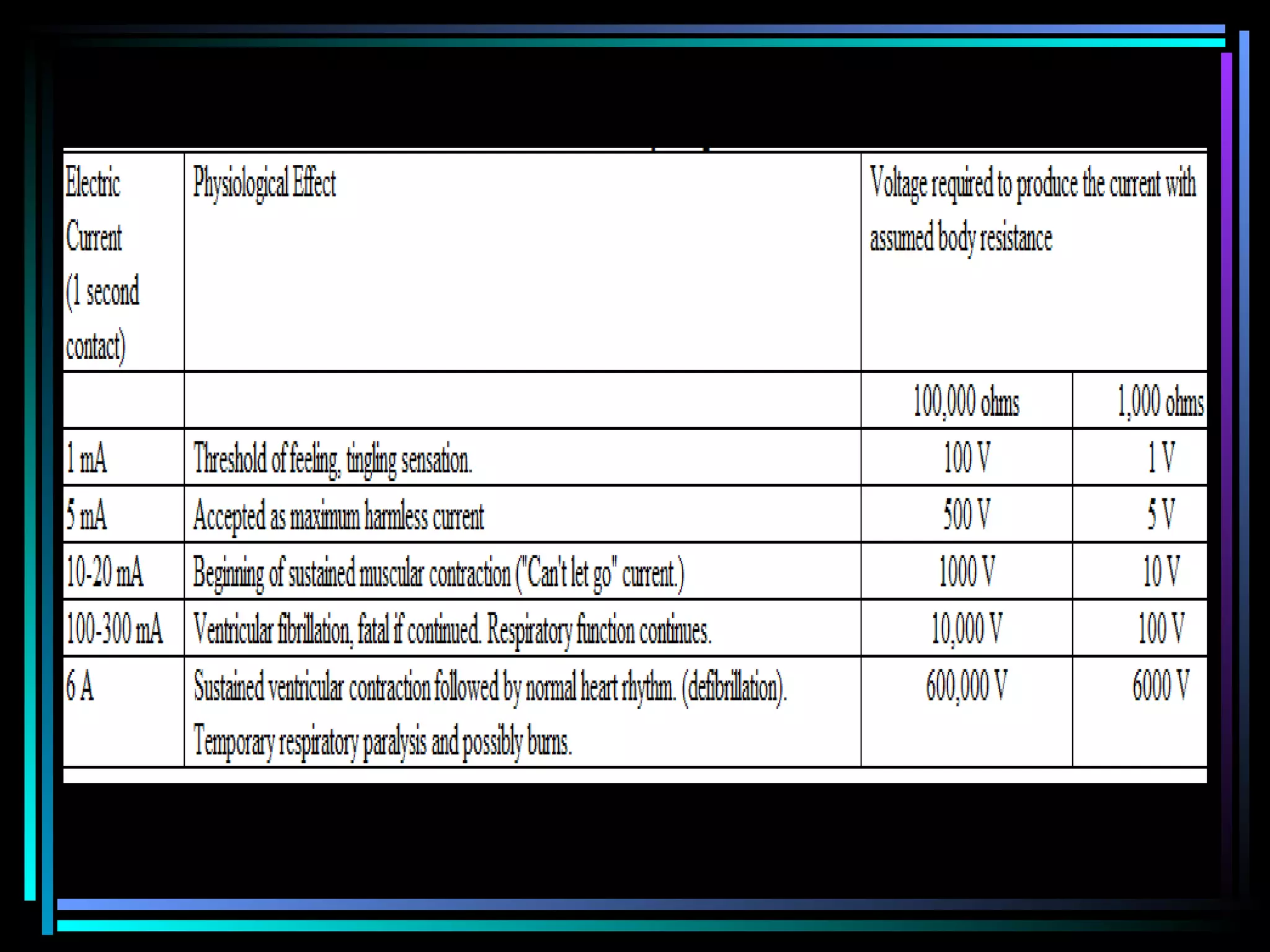
























This document provides information on electrical and lightning injuries, including: 1. The physics of electrical injuries and factors that determine injury severity such as voltage, current, resistance, and duration of contact. 2. The clinical features and effects on different body systems including the skin, heart, nerves and extremities. 3. The management of electrical injuries which involves monitoring, fluid resuscitation, wound care, and disposition depending on the severity of injuries.



















































![ELECTRICAL_AND_LIGHTNING[1] .6576875876587](https://cdn.slidesharecdn.com/ss_thumbnails/electricalandlightning1-250418104931-a1b02254-thumbnail.jpg?width=640&height=640&fit=bounds)





![4N[sic] - Electrocution](https://cdn.slidesharecdn.com/ss_thumbnails/4nsic-electrocution-161227134451-thumbnail.jpg?width=640&height=640&fit=bounds)





























