












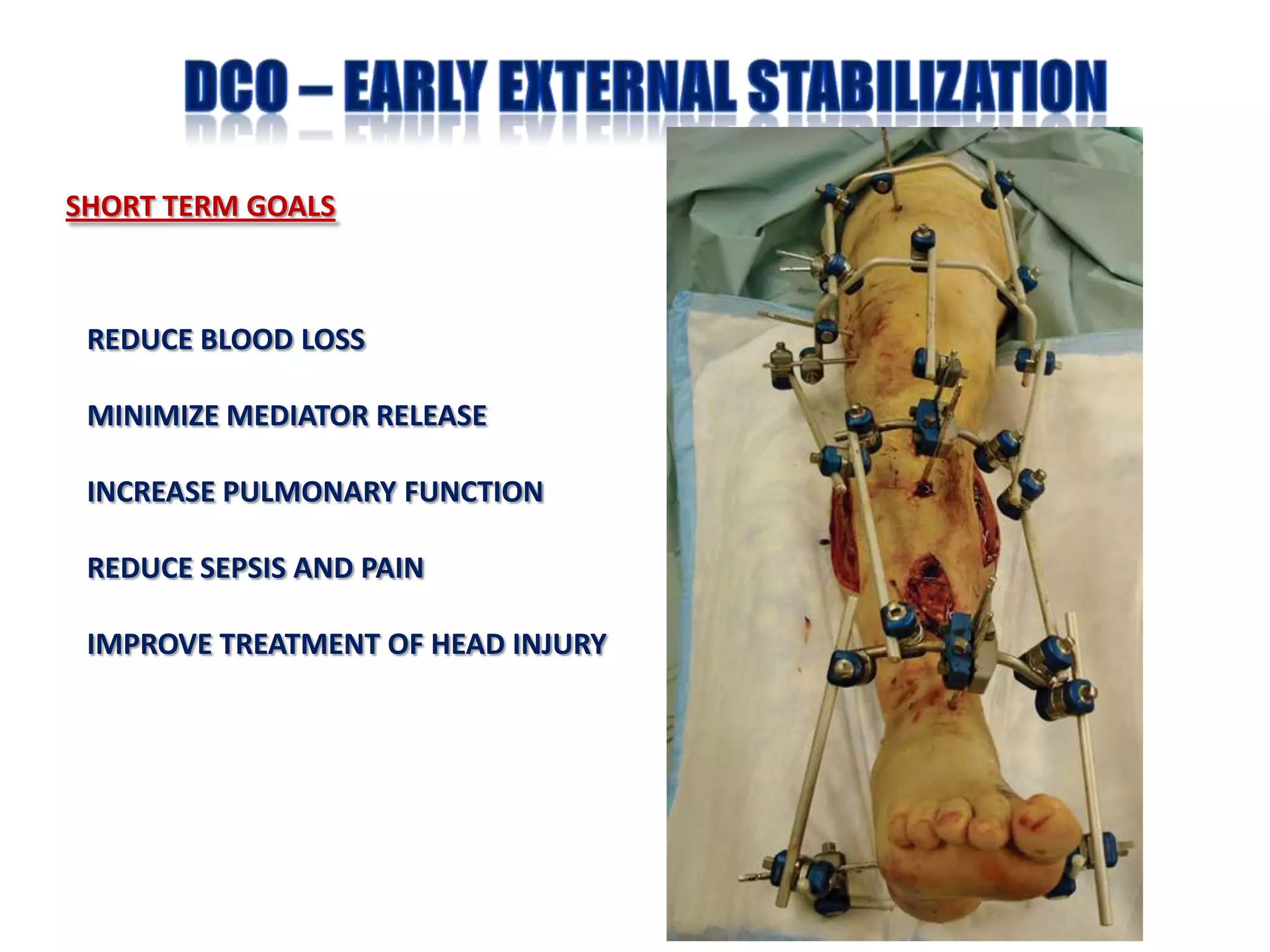







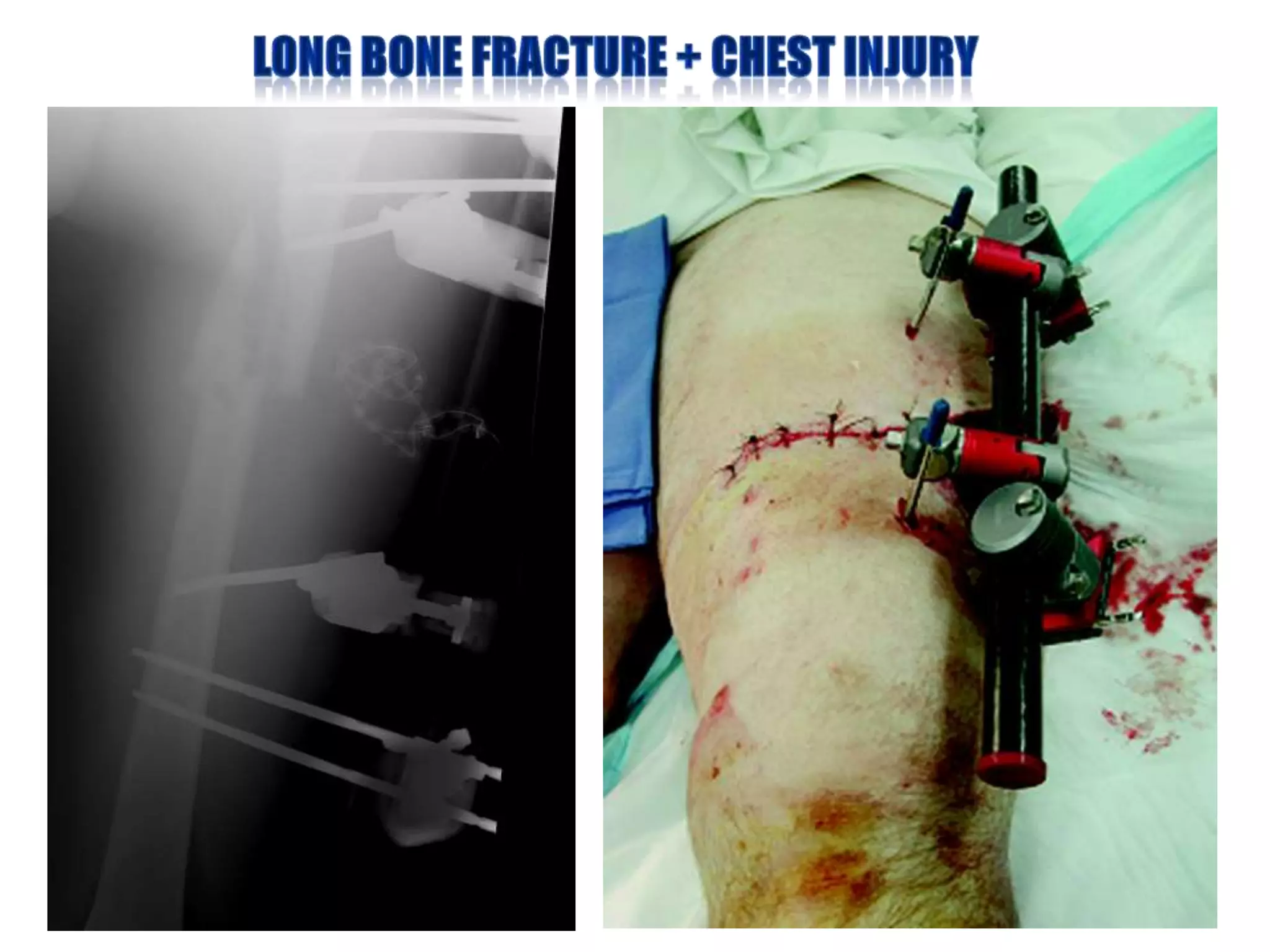



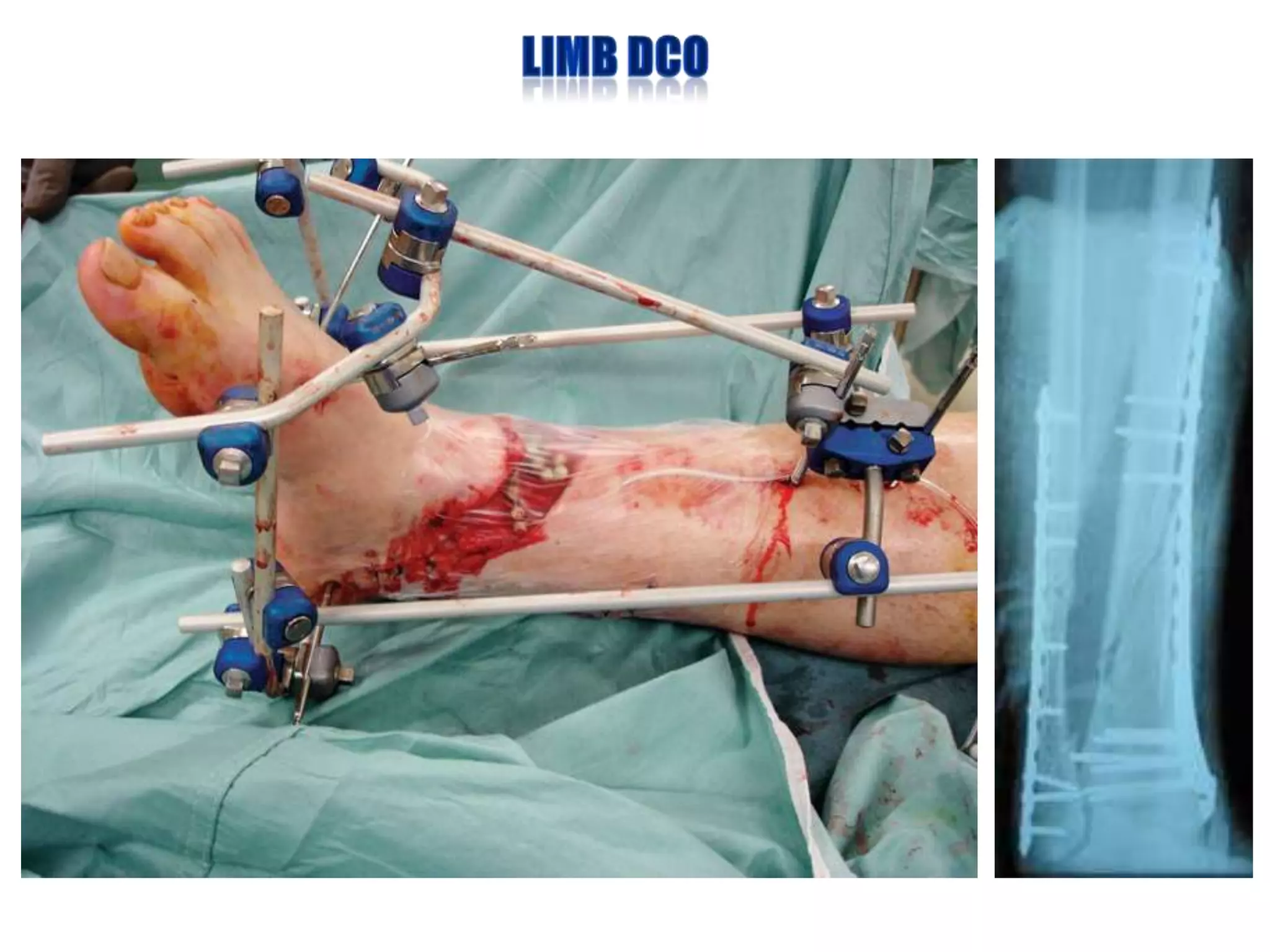


The document discusses the principles of damage control orthopaedics (DCO) in treating polytrauma patients. It notes that the goal of DCO is to stabilize orthopaedic injuries within 24-72 hours to prevent secondary complications, without causing additional physiological insult through early definitive surgery. It provides examples of when early fixation may be unsafe, such as in patients with severe chest or brain injuries, and recommends techniques like external fixation to temporarily stabilize fractures in these high-risk cases. The document emphasizes that the priority in polytrauma patients should always be to save the patient's life before definitively fixing fractures.



















































































