Downloaded 3,667 times

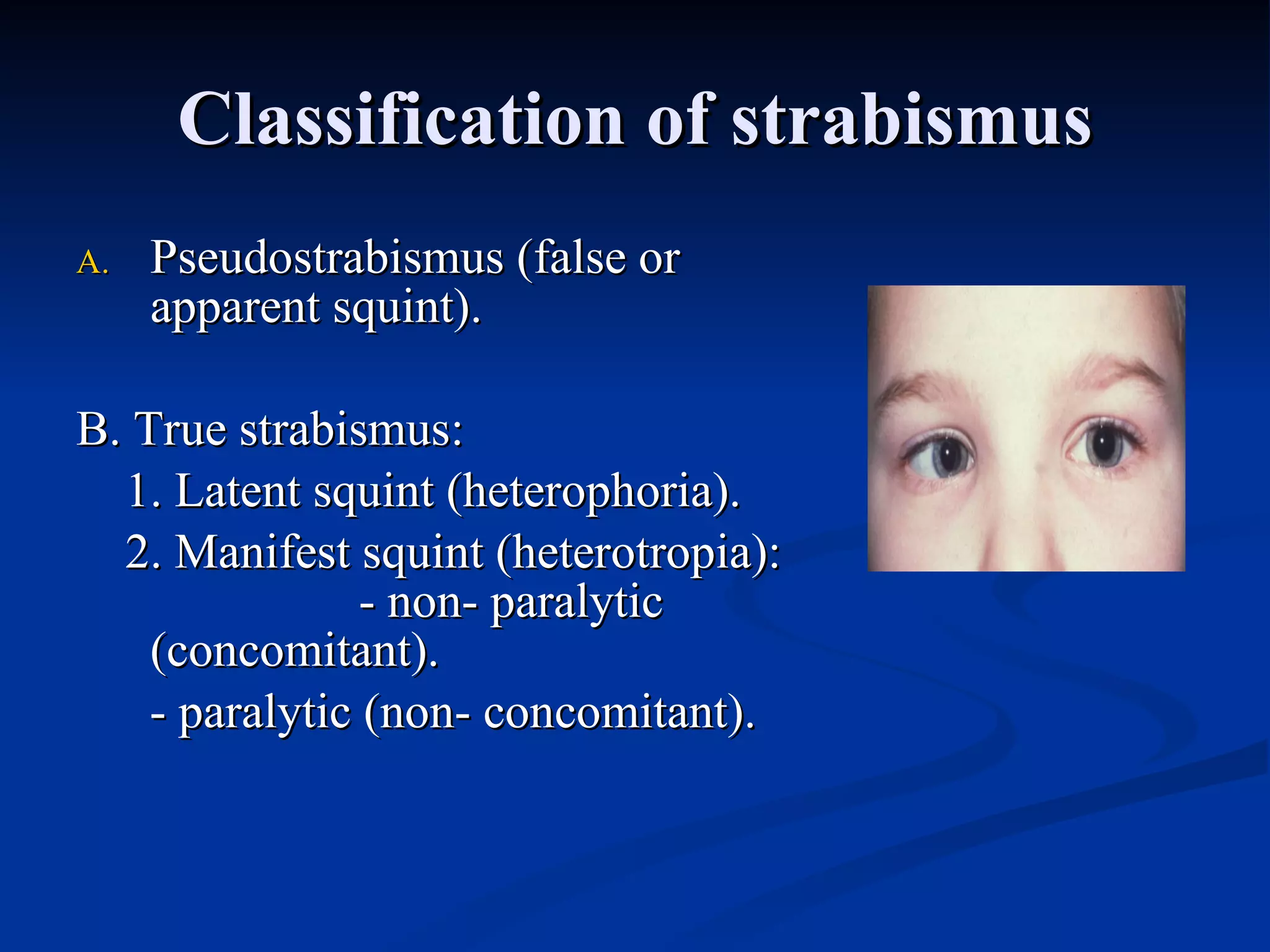



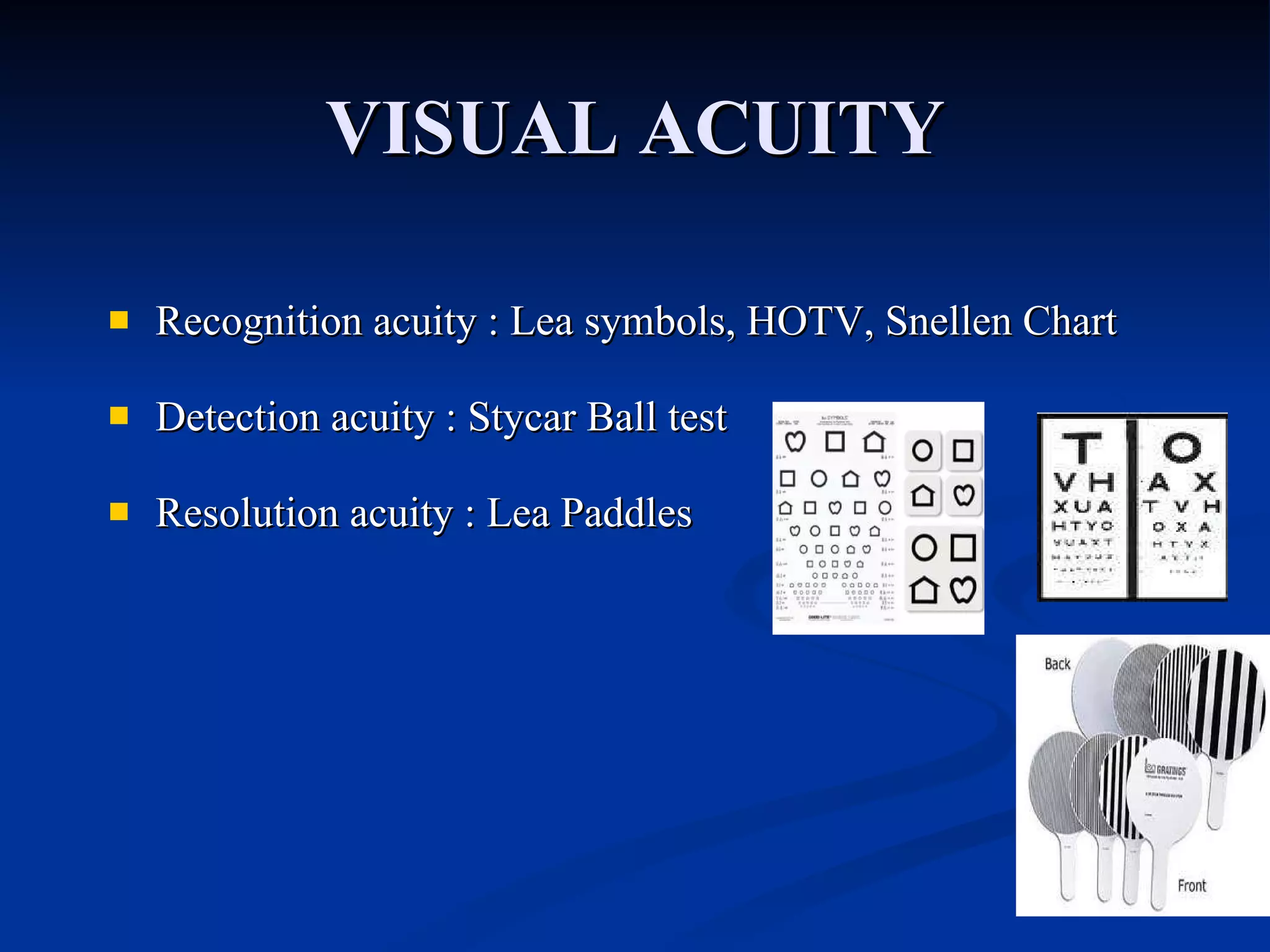



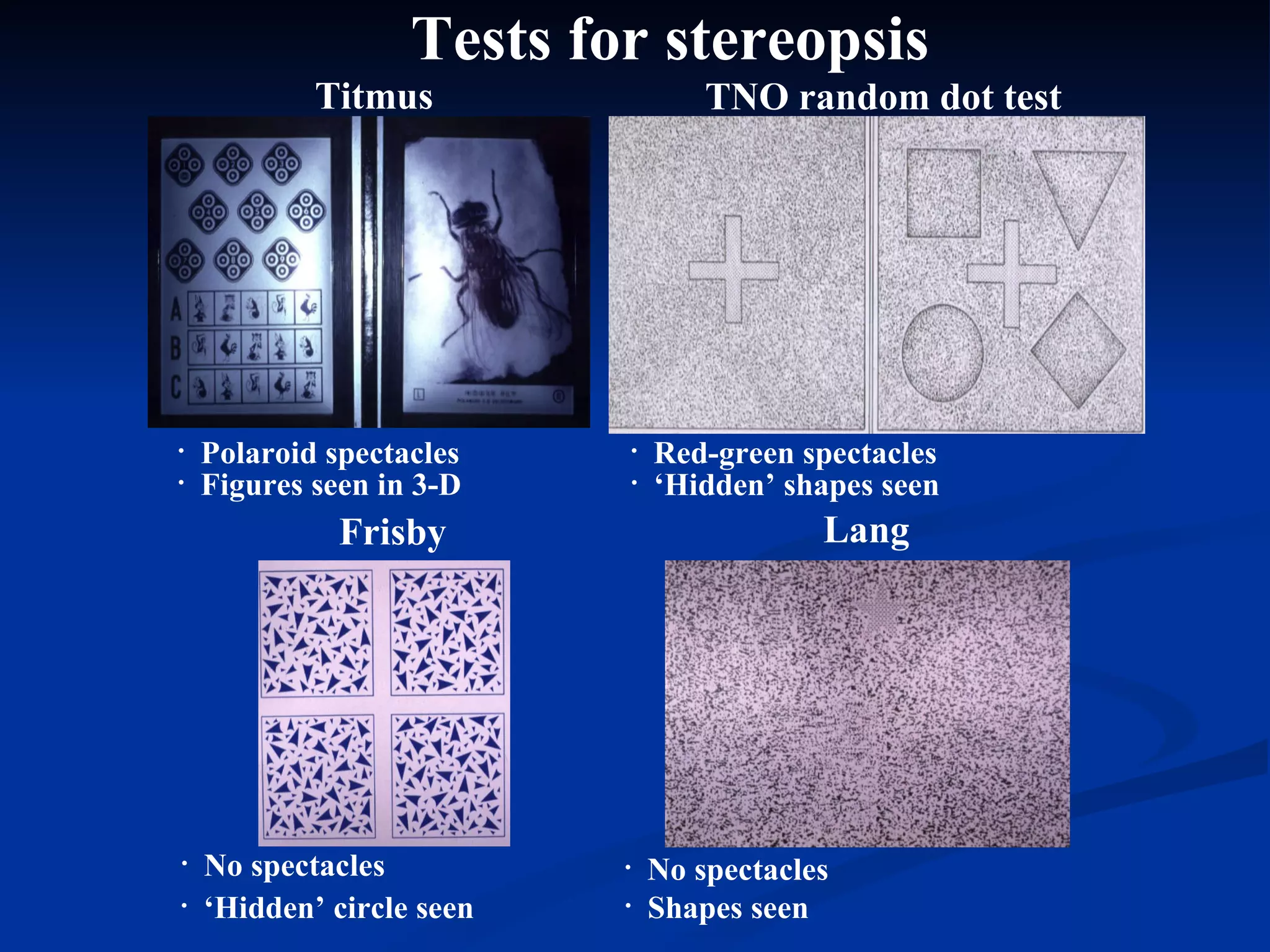
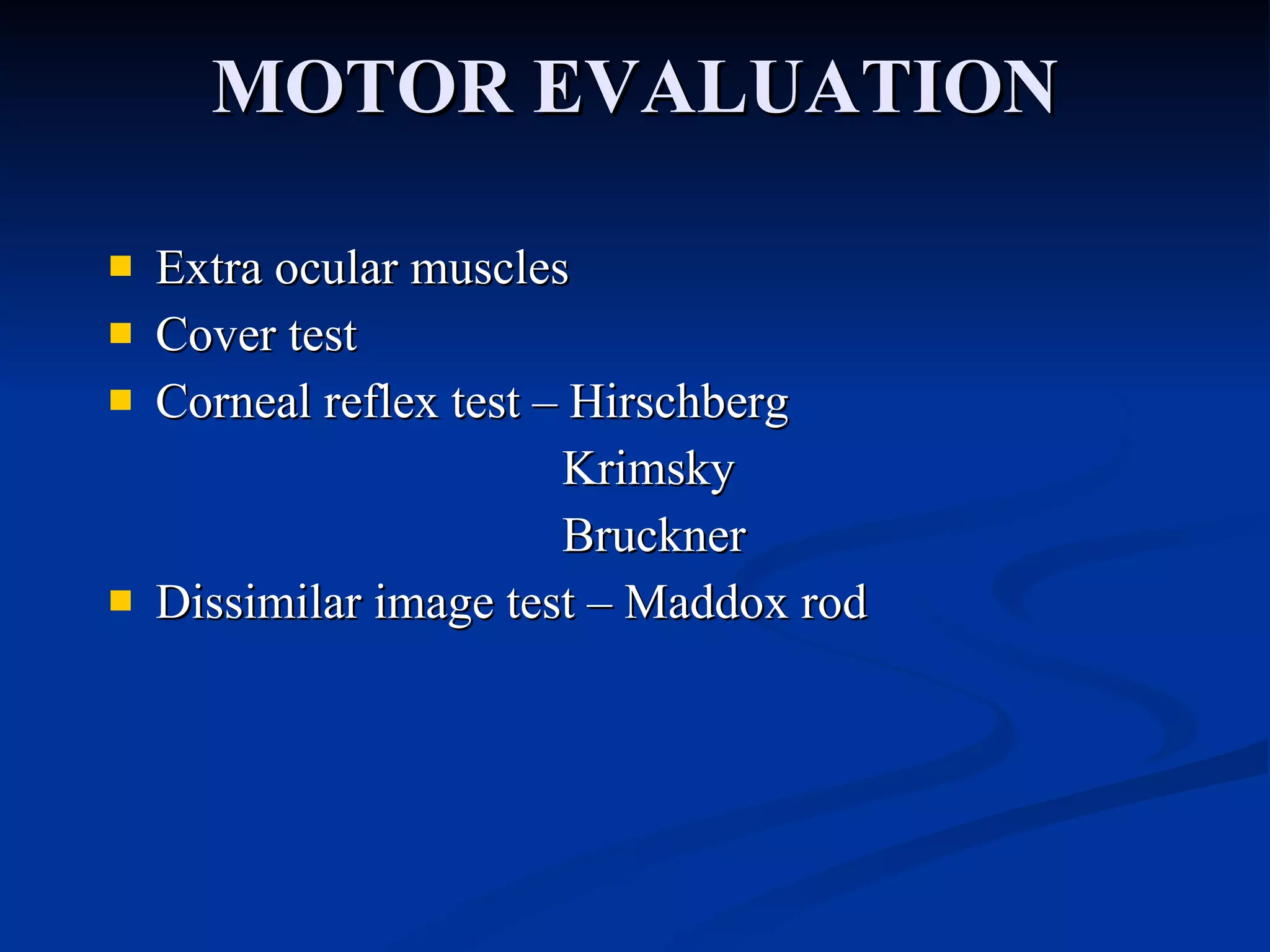



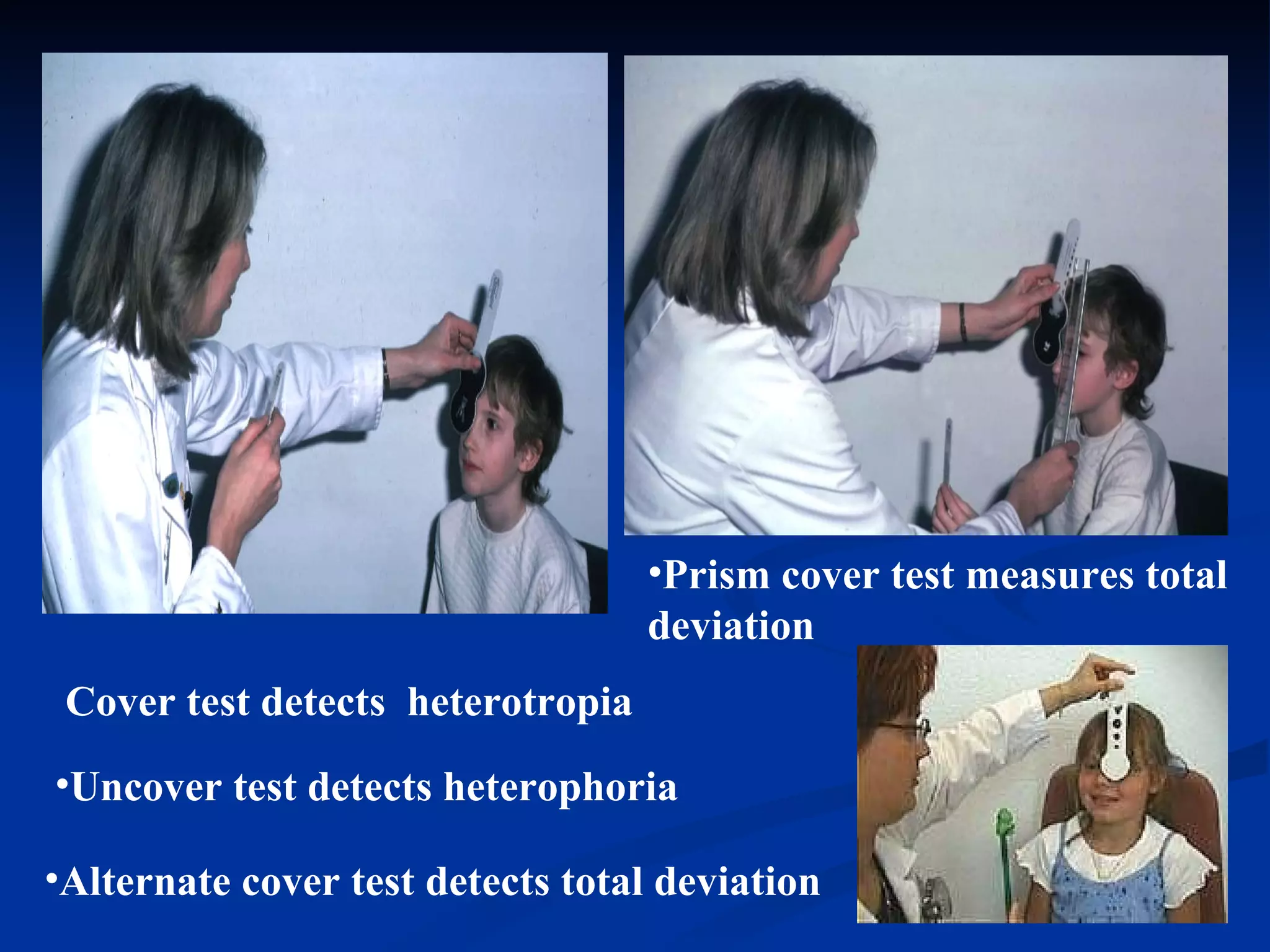

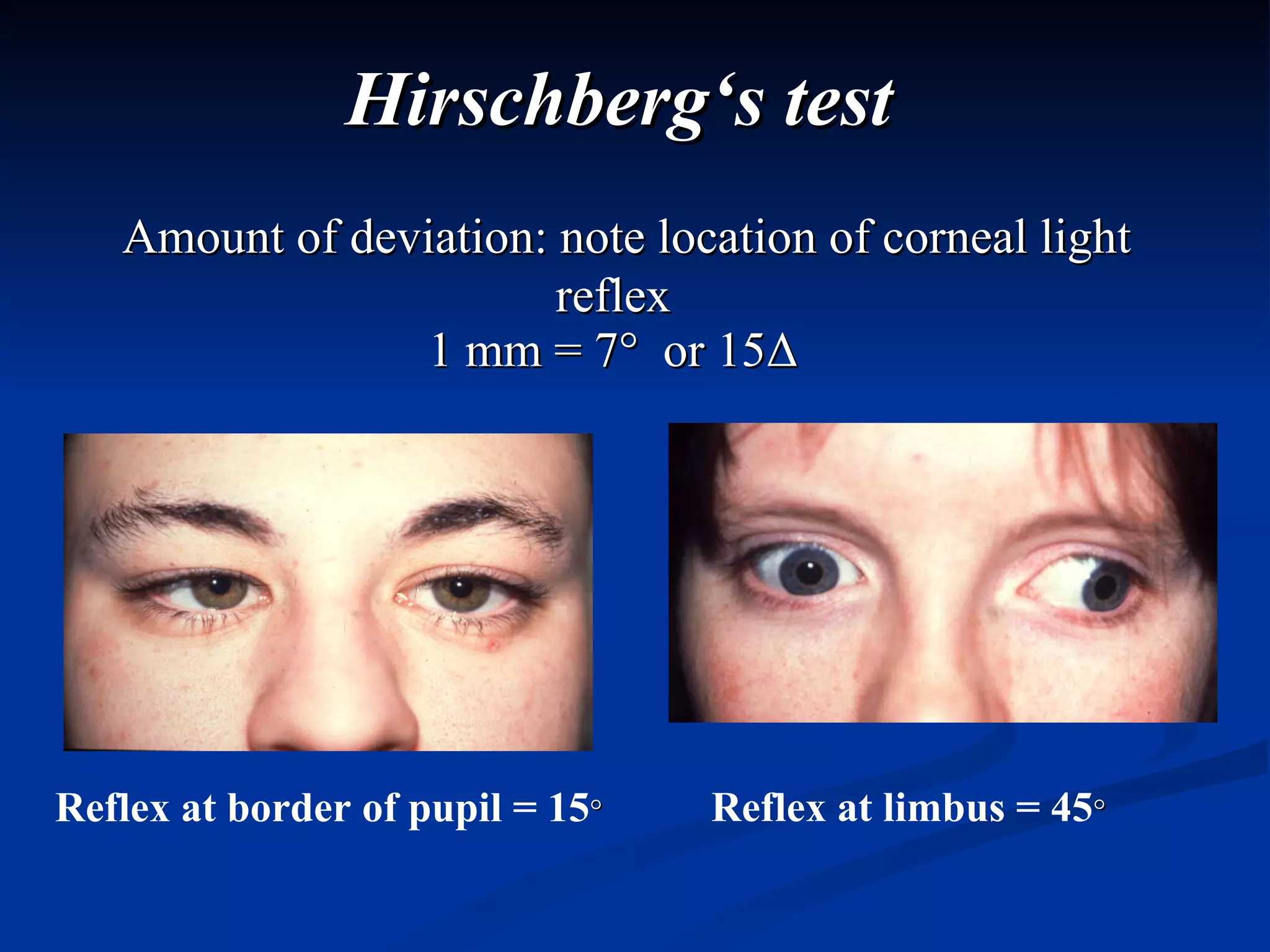
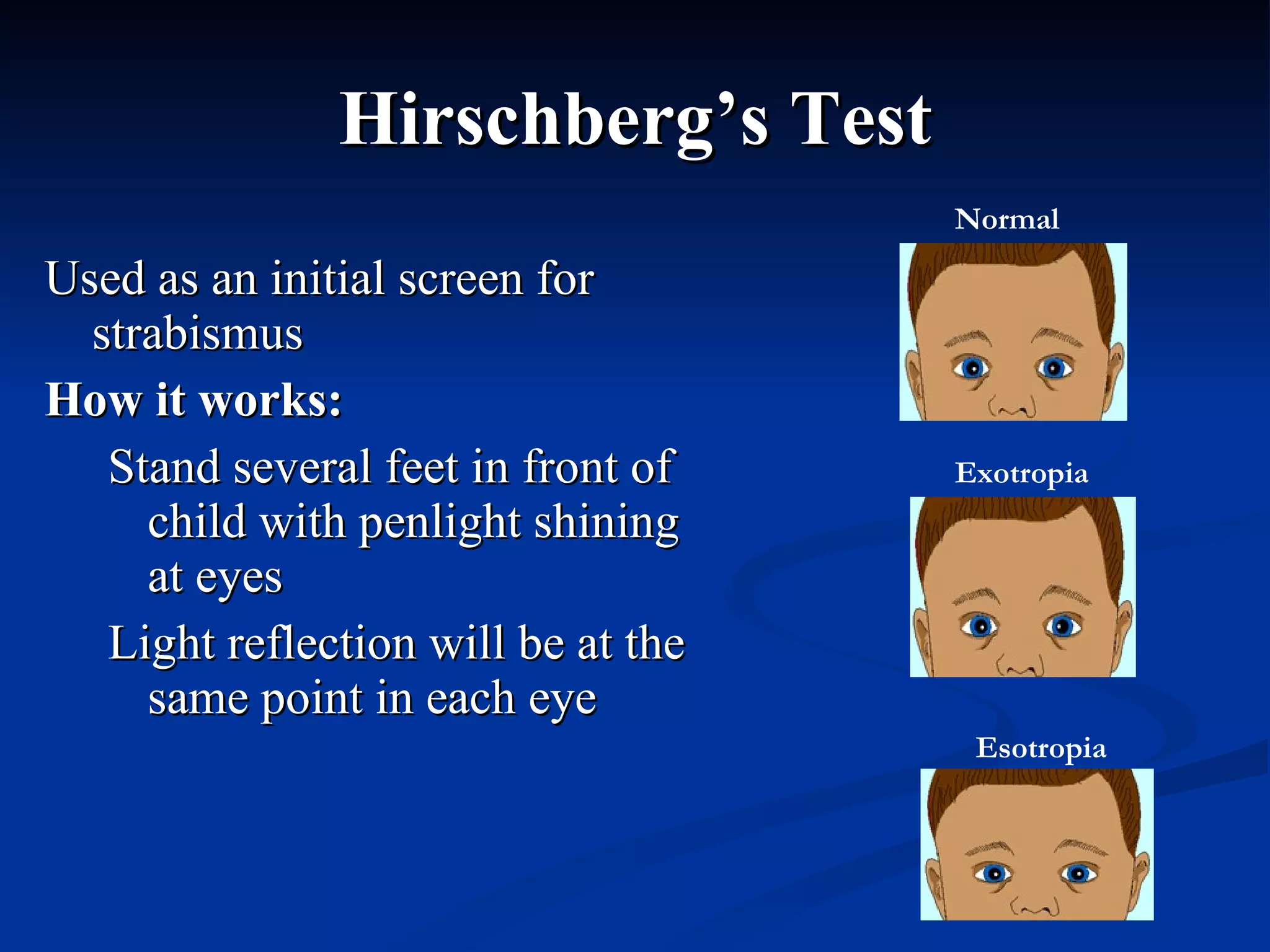


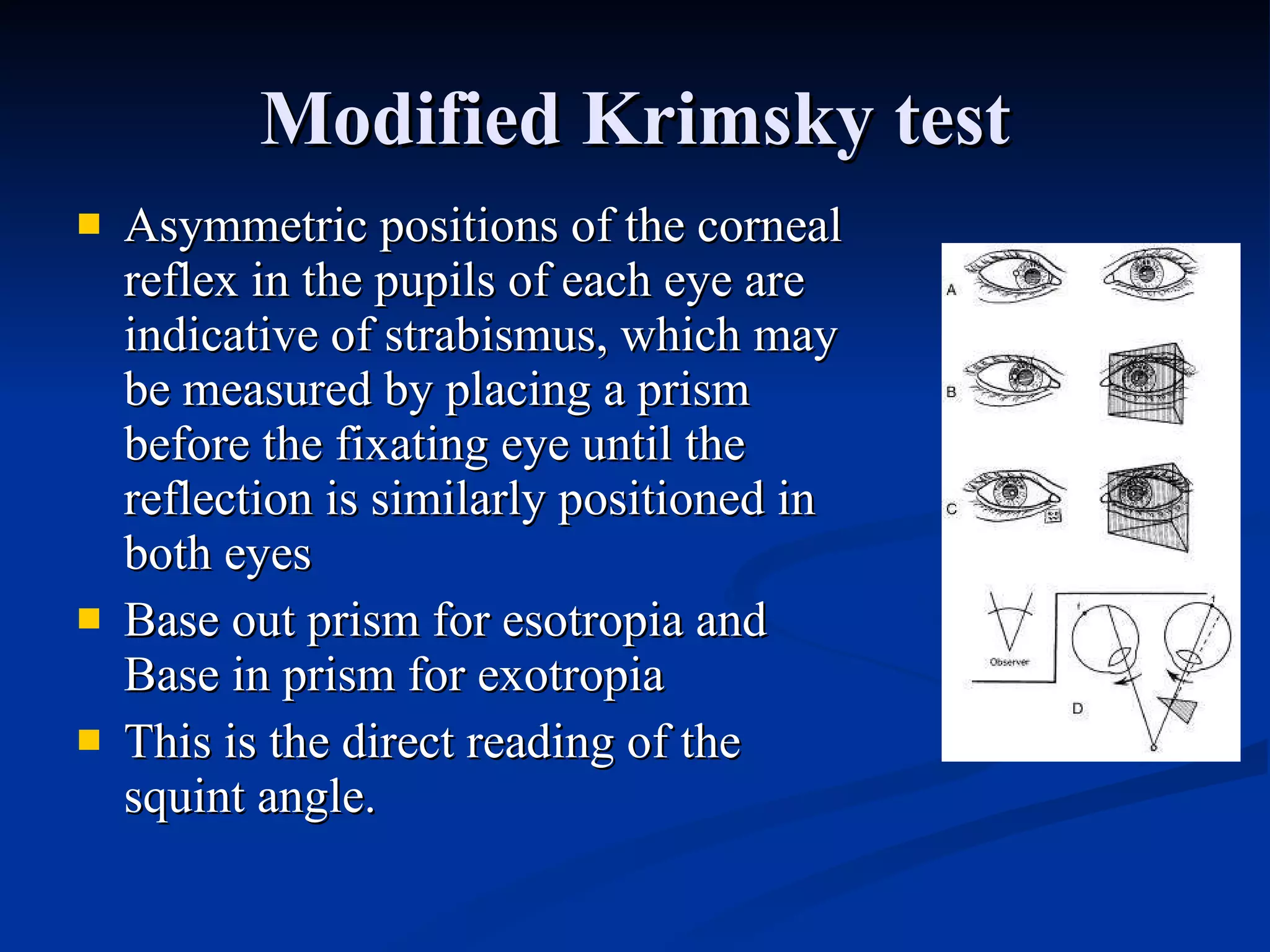
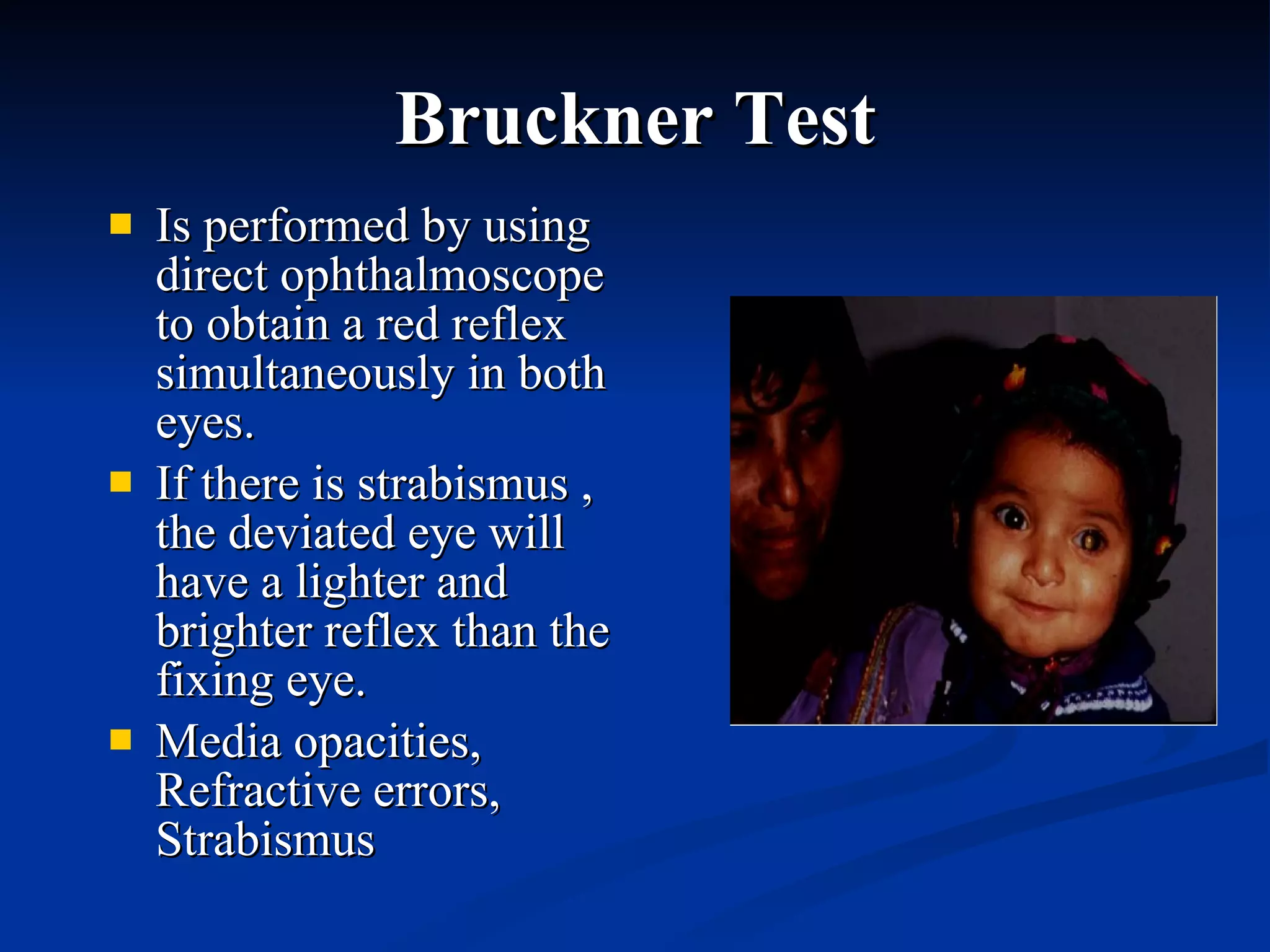





The document discusses the diagnostic evaluation process for strabismus. It covers the classification of strabismus, including pseudostrabismus and true strabismus. It also describes tests used to evaluate visual acuity, sensory function, motor function, and stereopsis. These include cover tests, versions, ductions, and specialized tests like Hirschberg's test, Krimsky test, and Bruckner test. The goal of the evaluation is to accurately diagnose the type of strabismus and measure the ocular misalignment.



































































