3. Dacryocystography (DCG)
•A Radiographic examination of the Nasolacrimal ducts
following administration of a contrast medium to
define the Lacrimal gland & NLD system anatomically
in search of stenosis or obstruction.
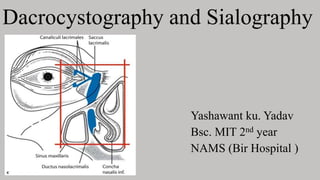
4. Anatomy glance
• The structure concerned with secretion & drainage of lacrimal or tear
fluid.
• Made up of following parts;
i. Lacrimal gland & duct.
ii. Conjunctival sac.
iii. Lacrimal puncta & lacrimal canaliculi
iv. Lacrimal sac.
v. Nasolacrimal duct.
6. Indications
Epiphora to demonstrate the presence and extent of obstruction
Obstruction may be due to:
congenital obstructions
supernumerary canaliculi
lacrimal fistula or diverticula
concretions (dacryoliths)
neoplastic or inflammatory processes
post treatment changes
8. Equipment
• Under couch image intensifier with digital imaging equipment to facilitate
production of subtracted image.
• Dedicated skull unit with focal spot size 0.3 mm to facilitate macro radiography.
Silver dilator and cannula lacrimal cannula or blunt needle with polythene
catheter
A 22 G/18G polyvinylchloride tubing catheter
The catheter technique has the advantage that the examination can be performed
on both sides simultaneously, and films can be taken during the injection.
Disposable syringe (3-5)ml
9. Contrast media
Oil based contrast media ,Lipiodol produces higher quality images of the lacrimal
sac than water-soluble dye
Low Osmolar CM [LOCM], 300mgI/ml
Dose: 0.5– 2 ml
Oil-soluble contrast media should not be utilized in the suspicion of tumors,
traumatism or fistulae, considering the risk of leakage and permanence in the
subcutaneous tissue for many years, inducing the formation of granulomas.
water-soluble contrast agents (iohexol , iopamidol , and 52.7% diatrizoate
meglumine and 26.9% iodipamide meglumine compared with the iodized oil-
based contrast agent Lipiodol.
10. Patients preparation
• Patient identification (3 'C's- correct patient, correct side, correct
procedure)
• Completed consent form
• No diet restrictions
• Collect/review relevant previous imaging for ease of access prior to
procedure
• A small quantity of local anesthesia is dropped into the inner canthus of
eye prior to cannulation of the punctum.
• Usually no premedication is given but children may require sedation.
12. Technique
• The patient lies supine on the fluoroscopy table with the head in a
reverse occipito-mental position.
• Support either side of the patient's head by immobilization device,
particularly if a subtraction technique is employed.
• Select a small field of view and fine focus
• Control images taken
13. Contd..
• Anesthetic eye drops are used for patient comfort
• A fine cannula is inserted into the puncta of each eye, then the eye is
closed and the catheter taped to the patient's cheek
• It may be necessary to dilate the puncta to facilitate insertion of the
cannula.
• After the mask is acquired, commence injection
• Images are taken immediately after injection
• A drainage image can be taken after 15 minutes if considered necessary
14.
15.
16. FILMS
Occipito mental –immediately following the injection to show filling and
emptying of the nasolacrimal duct
Lateral
When catheter is used
1st film-as plain film for subtraction
2nd film-when 1 ml of CM has been injected
3rd film-injection completed
The radiographs are then processed and subtracted
21. Technique Note
• It is normal practice to image both sides (comparison)
• It is preferable to inject both sides at the same time
• Collimate the X-ray beam to include the orbits superiorly and laterally
and the maxillary PNS inferiorly
• A focused spotlight can be a useful aid for the radiologist in locating
the lacrimal punctum
• Inferior punctum is often easier to cannulate
• Catheter should not be inserted too far into the canaliculus
• Dacrocystogram protocol may include adjunct nuclear medicine study
22. AFTER CARE
The eye is covered for approx. 1 hr after the examination to prevent ingress of
foreign material
Pt is usually kept in the department for about half an hour after the examination
until the effects of the LA is worn out.
24. SIALOGRAPHY
• A radiographic examination of the
salivary glands(PAROTID &
Submandibular GLAND) and
respectives ducts using contrast
media.
• Cannulation of Sublingual gland ducts
is almost impossible.
25. Anatomy
•3 pairs
1 . Parotid
2 . Submandibular
3 . Sublingual
• Situated adjacent to OC, aid in initial
digestion
26. Anatomy contd…
Parotid Submandibular Sublingual
Largest salivary gland Extends posteriorly from below
1st lower molar to angle of
mandible
Smallest pair
Lies just below the ZYG arch
in front & below the ear
Forms part of soft tissues on the
medial margin of the mandible & the
hyoid bone
Located in floor of mouth on
the surface of mylohyoid
muscle
Parotid duct(Stenson’s
duct) is 5cm long,
Submandibular duct(whartsons
duct ) is 5 cm long, runs
forward ,medially and upward
& opens into mouth on side of
frenulum
Numerous, small sublingual
ducts(ducts of Rivinus) open into
floor of mouth
runs over the messeter &
opens into oral vestibule
opposite 2nd upper molar
Ducts may join to form a
single(duct of Bartholin) which
empties into the submandibular
27. Indications
• Stones (Calculi) sialolithiasis
• Obstruction / Strictures
• Sicca syndrome
• Pain & Swelling (esp when recurrent)
• Infection
• Masses / Tumors
• Changes secondary to trauma
• When plain radiography is inconclusive
28. CONTRAINDICATIONS FOR EXAM
• History of contrast media allergies .
• Severe inflammation of the salivary ducts .
PATIENT PREPARATION:-
• Any radio opaque artefacts are removed
• Premedication usually not required but children may require sedation
29. Contrast media
• Oil based or water soluble contrast medium
• Dose:1 to 2 ml
• Either a compound with low viscosity or an ethiodized oil may be used
after the medium has been warmed to body temperature to further
reduce its viscosity.
• HOCM or LOCM 240 to 300 mgI/ml
30. Equipment
• Skull unit using macro radiography technique
• Fluoroscopic unit with spot film device
• lebrich’s double ended lacrimal probe
• Cannula 18G blunt needle and polythene catheter
• Disposable syringe 3-5ml
• Adhesive tape , cotton swabs , gauze piece, sterile gloves
• Lemon or ascorbic acid tablets to produce reflux stimulation of saliva before taking clear radiograph Overhead light
31. PRELIMINARY FILMS
Parotid gland Submandibular gland
AP view with head rotated 50 away from the
side under examination, Centre to the midline of
the lower lip
Inferosuperior using an occlusal film.
This is a useful view to show calculi.
Lateral, centered to the angle of the
mandible
Lateral, with the floor of the mouth depressed
by a wooden spatula.
Lateral oblique, centered to the angle of the
mandible, and with the tube angled 200
cephalad.
Lateral oblique, centred 1 cm anterior to the
angle of the mandible, and with the tube angled
200 cephalad
32. TECHNIQUE
• Preliminary radiographs
• Detect conditions that do not require contrast
• Give pt. secretory stimulant 2 to 3 minutes before contrast
administration
• Pt. asked to suck on lemon wedge -Opens duct for easy identification
• Duct orifice is sprayed with topical anesthetic
• Duct is cannulated, (dilator may be required), contrast introduced with
fluoroscopic guidance
• Contrast (oil based or water soluble iodinated) (conc = 240mg/ml)
• Should be injected manually until pt. feels discomfort
33. Contd..
• Quantity needed may vary between 1-2 ml
• Images taken immediately after contrast is complete
• After taking required images, pt. sucks on a lemon wedge again to
evacuate contrast
• Take post-procedure(delayed) radiographs after 5 minutes to confirm
evacuation of contrast/ demonstrate any residual contrast
34.
35. FILMS
Parotid----Control Films
• - AP - LAT - LAT OBLIQUE
Parotid -----Sialography Film
• - AP - LAT - LAT OBLIQU
SM----Control Films
• - INFEROSUPERIOR/OCCLUSAL
• - LAT
SM -----Sialography Film
• INFEROSUPERIOR/OCCLUSAL
• - LAT - LAT OBLIQUE
38. Filming of SM
Inferior superior
-Elevate the patient's thorax on
several firm pillows.
- Place the film in the mouth with the
long axis directed transversely.
- Central ray perpendicular to the
plane of the film
40. Contd..
• Center the IR to the inferior margin
of the angle of the mandible.
• Adjust the patient's head in a true
lateral position
• depressing the floor of the mouth
to displace the submandibular
gland below the mandible
• Neck should be hyper extended so
that the submandibular gland is
projected below the mandible
48. Contd..
• Sialography has also been recognized as a therapeutic
procedure because the dilation of the ductal system produced
during study may aid in the drainage of ductal debris
• Also, iodine which is used as a contrast media has beneficial
antiseptic properties
50. Ultrasonography
•Non invasive and cost effective imaging modality that can be
used in evaluation of masses occurring in the submandibular
gland and the superficial lobe of parotid gland
• best at differentiating between intra and extra glandular
masses and as well as between cystic and solid lesions
• Can demonstrate the presence of abscess in the acutely
inflamed gland also sialolithiasis
• The deep portion of the parotid gland is difficult to visualize
51. CT sialography
• CT is now well recognized and is of particular value in
distinguishing between lesions within two deep pole of the parotid
and with extrinsic pharyngeal masses which compress and displace
the gland
• Ultrafast CT and three dimensional –image CT sialography have
been effective for visualization of masses
• The disadvantage of CT includes radiation exposure, administration
of the contrast media for enhancement, and potential scatter from
dental restorations.
52.
53. MR sialography
• MR is used to diagnosis of lesions of the salivary glands
• Now contrast studies are useful in differentiating benign or low
grade malignant from the high grade malignant tumors
• Contrast enhancement is useful in differential diagnosis of cystic
from solid lesions, and when determining the degree of perineural
spread of malignant disease
54. Sequences used in MR sialography
•T1- weighted and T2-weighted images are taken with a slice
thickness of 3mm and interslice gap of 1mm.
•FSE T2-weighted image may require fat suppression
• Gadolinium enhanced scans with T1 weighting and fat
suppression are obtained in axial plane.
•Sagittal and coronal images may be obtained as required
58. Questions ?
• In sialography What are the filming sequences for parotid
and submandibular gland ?
• What are the time for delay radiograph in both DCG and
SCG ?
• List out the anatomic structure of lacrimal apparatus ?
• Basic Sequence used in MRI for sialography
• What is the advantage of catheter technique in DCG? And
what is the volume of contrast used in DCG?
Editor's Notes
-paired, almond-shaped, serous gland.
-situated in lacrimal fossa on the anterolateral
-Small accessory lacrimal glands are also found around it
-About 10-12 of its duct pierce conjunctiva of upper lid & open into conjunctival sac near the superior fornix
-Potential space between palpebral & bulbar part. (Conjunctival sac)
-small aperture, in medial portion of each eyelid.
Collect tears produced by lacrimal glands.
Canaliculus begins at the lacrimal puncta, about 10mm long.
Has vertical part, 2mm long & horizontal part, 8mm long.
-Membranous sac 12mm long & 5mm wide
-Inflammation of sac called dacrocystitis.
-Membranous passage 18mm long.
Runs downward, backward & laterally and opens into inferior meatus of nose
Anesthetic eye drops(0.4% benoxinate hydrochloride) can be used for patient comfort.
Local anesthesia
Other modalities
Ct
Mri
Sicca syndrome: An autoimmune disease, also known as Sjogren syndrome, that classically combines dry eyes, dry mouth, and another disease of connective tissue such as rheumatoid arthritis (most common), lupus, scleroderma or polymyositis.
Lupus is a systemic autoimmune disease that occurs when your body's immune system attacks your own tissues and organs.
Polymyositis: a rare inflammatory disease that causes muscle weakness affecting both sides of your body.
Center the horizontal ray to the parotid area
Center to a point approximately 1 inch (2.5 cm) superior to the mandibular angle.
Adjust the head so that the midsagittal plane is rotated approximately 15 degrees toward the IR from a true lateral
-An oblique projection is often necessary to obtain an image of the deeper portions of the parotid gland
-20 to 25 degree cranial angulation is given
Post secretory films
Same views are taken 5 min after the cannula is taken out to see the emptying of the duct with the same views
Also its been beneficial for the patient who are unable to lie for a long time (pediatric, claustrophobic, physically or mentally challenged patients) and for the patients for whom MRI is contraindicated
Ap/ lat / oblique
inferosuperior occlusal
15min/5 min
Lacrimal gland in lacrimal fossa . Lacrimal ducts . Conjunctival sac , puncta 10 mm . Nasolacrimal sac and duct in inferior nasal meatus
T1W/T2W/ FSE T2W for fat suppression or STIR
0.5-2 ml (300mgI/ml)