Downloaded 238 times


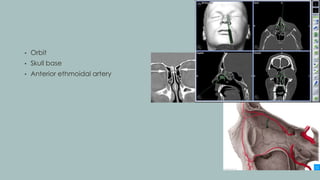

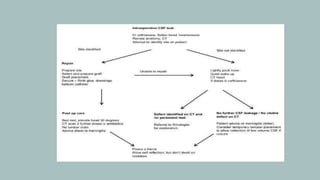
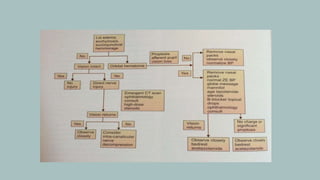


The document outlines essential guidelines for preventing complications during endoscopic sinus surgery, focusing on anatomical considerations and proper surgical techniques. It highlights the importance of preoperative preparation, identifying anatomical landmarks, and understanding potential complications, which range from minor issues like orbital hematoma to major risks such as hemorrhage and blindness. Clinical scenarios illustrate the complexities involved in managing complications and the necessary proactive measures to minimize risks in patients undergoing surgery.















































































