Development of Hepatic and Biliary Systems (HBS
•
14 likes•4,121 views

This document summarizes the development of the human biliary system and liver. It describes how the septum transversum forms an initial partition in the body cavity. It also discusses how the hepatic bud develops from the foregut and grows into the septum transversum, forming the liver and gallbladder. The vitelline and umbilical veins break down within the septum transversum to form the liver sinusoids. The document concludes by outlining some common congenital anomalies that can occur in the development of the biliary system and liver.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Development of Hepatic and Biliary Systems (HBS
Similar to Development of Hepatic and Biliary Systems (HBS (20)
More from Prabhakar Yadav
More from Prabhakar Yadav (20)
Recently uploaded
Recently uploaded (20)
Development of Hepatic and Biliary Systems (HBS
- 1. DEVELOPMENT OF HBS Dr. Prabhakar Yadav Associatet Professor Department of Human Anatomy B.P. Koirala Institute of Health
- 2. Septum Transversum: Appears on day 22 as a thickened bar of mesoderm lying between cardiogenic area & cranial margin of embryonic disc . Cephalic folding carries this bar ventrally & caudally until it is wedged between cardiogenic area and neck of yolk sac It forms initial partition separating coelom into thoracic & abdominal cavity and give rise to part of diapharagm and ventral mesentry of stomach and duodenum
- 3. Stomach is seen as fusiform dialation . Dorsal border is attached to posterior abdominal wall by fold of peritoneum – dorals mesogastrium Ventral boder is attached to septum transversum by fold of peritoneum- ventral mesogastrium
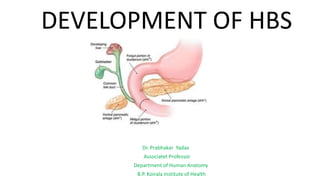
- 4. Liver primordium: Thrird week Outgrowth of endodermal epithelium (hepatic diverticulum or liver/ Hepatic bud) from the ventral aspect at the distal end of foregut, just at its junction with the midgut. Hepatic bud consists of rapidly proliferating cells that grows into the ventral mesogastrium and through it into the septum transversum. Bud divides into two parts: large cranial part - pars hepatica (liver )& small caudal part - pars cystica (gallbladder & cystic duct). Part of bud proximal to pars cystica forms common bile duct (CBD).
- 6. Pars hepatica divides into right and left portions to form right and left lobes of the liver. Initially both lobes of the liver are of equal size. As right &left portions of pars hepatica enlarge, they extend into septum transversum. The cells arising from them form interlacing hepatic cords (cords of hepatocytes). In this process, vitelline and umbilical veins present within the septum transversum get absorbed and broken to form the liver sinusoids.
- 8. Vitelline Veins: arise from yolk sac & pass to the sinus venosus. When the yolk sac disappears vetelline veins pass on either side of duodenum to form plexus around it and open in corresponding horn of the sinus venosus. Before opening in the sinus venosus, they pass through septum transversum. As Liver cords growing into the septum transversum, portions of vitelline veins as well as umbilical veins passing through the septum transversum break up and form extensive vascular anastomosis— liver(hepatic) sinusoids.
- 9. • Cells of hepatic cords later become radially arranged in hepatic lobules. • Bile canaliculi and ductules are formed in liver parenchyma and establish connections with extrahepatic bile ducts • The oxygen-rich blood supply and proliferation of hemopoietic tissue are responsible for the massive enlargement of the liver • Due to rapid enlargement, liver occupies major portion of the abdominal cavity forcing the coils of the gut to herniate through umbilicus (physiological hernia).
- 10. Liver: Three sources: 1. Parenchyma of liver - from endodermal hepatic bud of foregut. 2. Fibrous stroma of liver- from mesenchyme of septum transversum, 3. Sinusoids of liver -From absorbed & broken vitelline & umbilical veins within the septum transversum. • Liver is an important centre of hemopoiesis - begins at about the sixth week of IUL and continue till birth. • Hepatocytes start secreting bile at about twelfth week of IUL. • Bile enters intestine and imparts a dark green color to first stools (meconium) passed by newborn
- 11. Congenital anomalies Riedel’s lobe: Tongue-like extension of normal hepatic tissue from the inferior margin of the right lobe of the liver. Polycystic disease of the liver: -Biliary tree within the liver (bile canaliculi and bile ductules) normally connects them with extrahepatic bile ducts. - Failure of union of some of these ducts may cause the formation of cysts within the liver. - Usually associated with cystic disease of kidney and pancreas.
- 12. 3. Intrahepatic biliary atresia: cannot be subjected to surgical correction. - liver transplant of the child ; -let the child die. 4. Caroli’s disease: congenital dilatation of intrahepatic biliary tree- lead to the formation of sepsis, stone, and even carcinoma.. 5. Others: Rudimentary left lobeof liver, Absence of quadrate lobe Presence of accessory liver tissue in falciform ligament
- 13. Development of Gallbladder and Extrahepatic Biliary Ducts (Extrahepatic Biliary Apparatus) • Gallbladder & cystic duct develop from pars cystica. • Part of hepatic bud proximal to the pars cystica forms CBD.
- 14. • Initially the CBD/bile duct opens on the ventral aspect of developing duodenum. • as the duodenum rotates, opening of CBD is carried to dorsomedial aspect of the duodenum along with ventral pancreatic bud. Initially extrahepatic biliary apparatus is occluded with epithelial cells. Later it is recanalized by vacuolation resulting from degeneration of the cells
- 15. Anomalies of the extrahepatic biliary apparatus: Anomalies of gallbladder: • Agenesis of gallbladder : pars cystica from the hepatic bud fails to develop. • Absence of the cystic duct(sessile gallbladder ): occurs when pars cystica form gallbladder that drains directly into CBD. Anomalies of shape • Phrygian cap: occurs when fundus of the gallbladder folds on itself to form a cap-like structure
- 16. • Hartmann’s pouch: is formed when the posterior medial wall of the neck (infundibulum) of gallbladder projects downward. - pouch may be adherent to the cystic duct or CBD. • Septate gallbladder and double gallbladder: Gallbladder may be partially or completely subdivided by a septum. Some time it may be partially or completely duplicated.
- 17. • Anomalies of the positions: • Gallbladder may lie transversally on the inferior surface of the right or left lobe of the liver. • Intrahepatic gallbladder: gallbladder is embedded within the substance of the liver. • Floating gallbladder: Gallbladder is completely surrounded by peritoneum and attached to the liver by a fold of peritoneum (mesentery)
- 18. Anomalies of extrahepatic biliary ducts : Occur due to failure of recanalization of these ducts. • Atresia of bile duct • Atresia of entire extrahepatic biliary duct system • Atresia of common hepatic duct • Atresia of hepatic ducts atresia of the bile duct manifests as persistent progressive jaundice of newborn and may be associated with the absence of the ampulla of Vater
- 19. Accessory bile ducts: may open directly from the liver into the gallbladder. There may be leakage of bile into the peritoneal cavity after cholecystectomy if they are not recognized at the time of surgery. Choledochal cyst: develops due to an area of weakness in the wall of bile duct. It may contain—2 L of bile and thus may compress the bile duct to produce an obstructive jaundice. Moynihan’s hump: In this condition, the hepatic artery lies in front of the common bile duct.
- 20. THANK YOU