Call Girls Service Pune Vaishnavi 9907093804 Short 1500 Night 6000 Best call ...
Omgb
1.
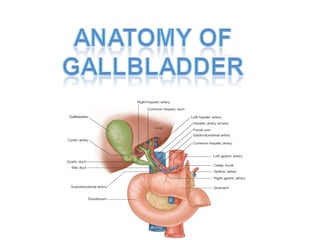
2. The gallbladder is a pear-shaped sac lying on the
visceral surface of the right lobe of the liver in a fossa
between the right
and quadrate lobes.
Size: 10 x 4 cm
(but depends
on volume of bile)
Volume: 35-50 ml
Thickness: 1-2 mm
3. Parts
• Distal fundus: extends
beyond anterior liver
margin.
• Central body: most of
gallbladder.
• Neck: narrows as it
joins the cystic duct.
• Infundibulum: portion
of body that joins the
neck.
5. Vasculature
cystic artery, usually
a branch of right
hepatic artery.
Note: variations of
bile ducts and
arteries may be
dangerous during
surgery.
6. Embryology
Develops with bile duct and
liver during week 4 as
ventral bud (hepatic
diverticulum) from caudal
foregut .
Hepatic diverticulum has two
components:
pars hepatica and
pars cystica .
Parts hepatica gives rise to
liver, common hepatic duct
and intrahepatic bile ducts.
7. • Pars cystica gives rise to cystic diverticulum, which
gives rise to gallbladder and cystic duct.
• Hepatic diverticulum elongates to form common
bile duct.
• Above structures begin as solid cords, but at 8
weeks have lumina.
9. Agenesis (absence)
• Rare; 50% discovered at autopsy.
• Usually no cystic duct either .
• Associated with choledocholithiasis, duodenal
atresia and other congenital anomalies.
Hypoplasia
• Associated with extrahepatic biliary atresia.
Micro gallbladder
• Defined as less than 2-3 cm long, 0.5 -1.5 cm wide .
• Associated with idiopathic neonatal hepatitis,
alpha-1-antitrypsin disease, cystic fibrosis.
10. Cysts
• May begin as pseudodiverticula (Rokitansky-Aschoff
sinuses) with progressive occlusion of
communication with gallbladder.
Diverticula
Heterotopia
• Also called ectopia or choristoma .
• Normal tissue in abnormal location.
• Includes liver parenchymal nodules, usually 2.5 cm
or less, suspended to gallbladder by mesenteric
stalk.
11. Hourglass gallbladder
• Divided by central constriction.
Wandering gallbladder/ Floating gall bladder
• Long mesentery or no firm attachment to liver.
• At risk for torsion.
Abnormal positions
• Left sided (with or without situs inversus)
• intrahepatic
• retroperitoneal
• suprahepatic
• also within falciform ligament, lesser sac or
12. Phrygian cap
• Inversion of distal fundus
into body, to which it may
become adherent.
• Either anatomic variant or
acquired abnormality.
• Present in 5% of
cholecystograms.
13. Double gall bladder
Absence of the cystic duct
Low insertion of the cystic duct
An accessory cholecystohepatic
duct