Download as PPSX, PPTX



























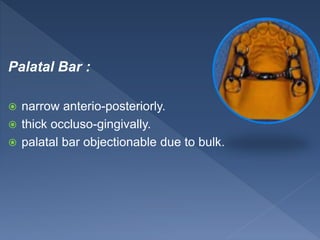





The document details the components and design considerations for partial dentures, focusing on connectors that unify and stabilize the prosthesis while addressing stress distribution and soft tissue interference. It discusses different connector shapes such as bars and straps, their positional requirements, and contraindications for use in various clinical scenarios. Lastly, it highlights specific designs and their indications in relation to patient anatomy and remaining teeth.














































































