Download as PPSX, PPTX





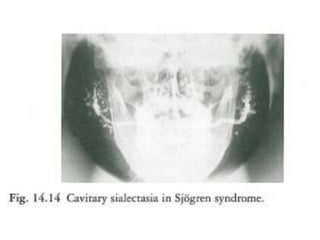
![• Other investigations useful in assessing the
degree of salivary gland involvement include
estimation of parotid salivary flow rates, which
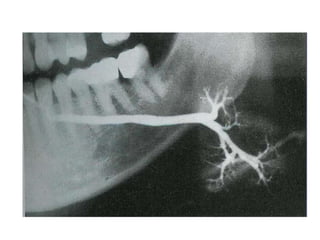
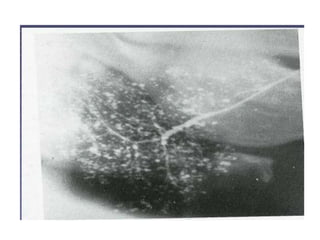
are usually reduced, and sialography, which
shows varying degrees of sialectasis often
producing a 'snowstorm' or 'cherry tree in
blossom'-like appearance.
• Salivary scintiscanning using [99Tcm]
pertechnetate is also of value. The radioisotope
is concentrated in salivary glands and its
uptake is reduced in patients with Sjogren
syndrome.](https://image.slidesharecdn.com/diseases-of-salivary-glands1-181028212353/85/Diseases-of-salivary-glands-59-320.jpg)

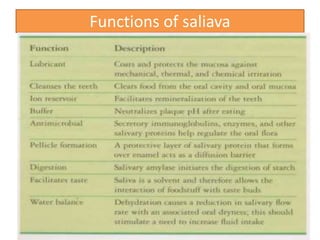
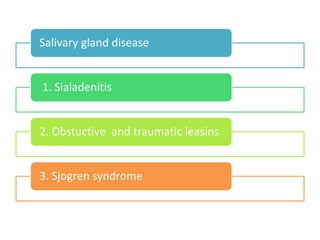
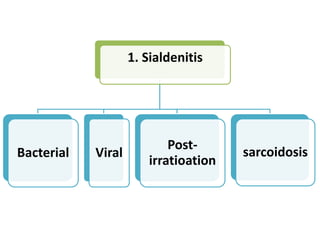
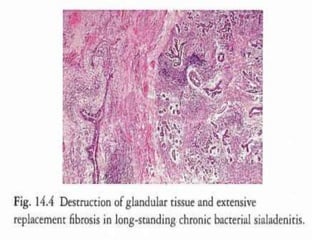
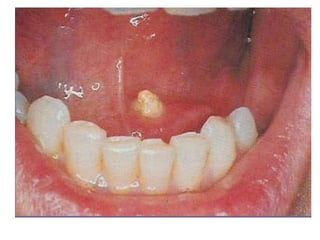
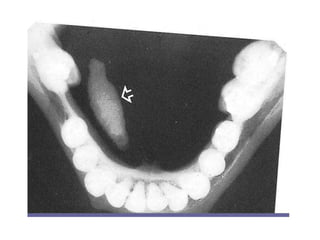
This document discusses diseases of the salivary glands, including sialadenitis (inflammation of the salivary glands), which can be caused by bacterial or viral infections. It also discusses Sjogren's syndrome, an autoimmune disease that causes dry mouth and dry eyes due to lymphocytic infiltration and destruction of the lacrimal and salivary glands. Obstructive diseases like salivary calculi (stones) are also covered. The document provides details on symptoms, diagnosis, and treatment of various salivary gland diseases.














































































