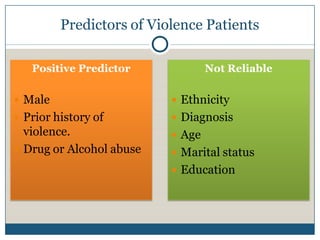
The highest risk areas for workplace violence are the emergency department, psychiatric wards, and waiting rooms. 70% of incidents go unreported, and women are over 8 times more likely to be victims. Hospitals should implement security measures like metal detectors, restrict access, and train staff in de-escalation techniques to help prevent and manage violent situations. An ounce of prevention is worth a pound of cure.




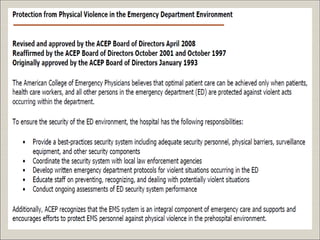
![American College of Emergency Physicians. Emergency physicians’ patient care
responsibilities outside of the emergency department [policy statement];
Approved September 1999. Ann Emerg Med 2000;35:209](https://image.slidesharecdn.com/workplaceviolence-091111102718-phpapp02/85/Workplace-Violence-34-320.jpg)



































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









