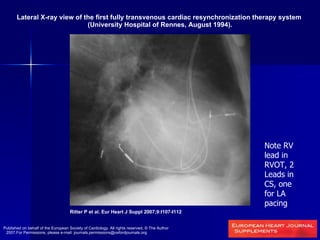
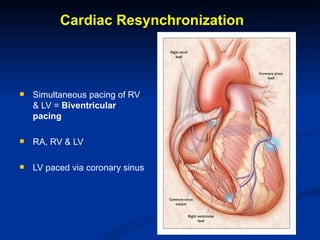
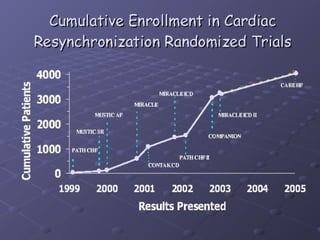
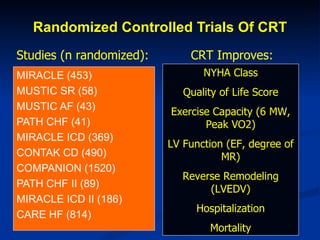
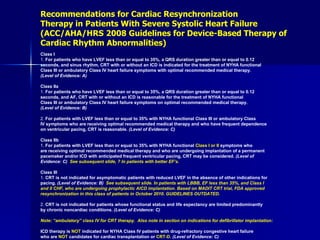
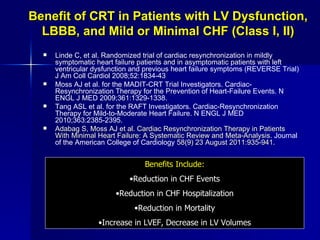
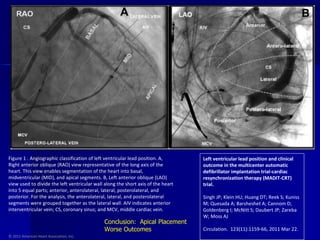
This document discusses the history and evidence for cardiac resynchronization therapy (CRT). It notes that approximately 25% of heart failure patients have intraventricular conduction delays that cause dyssynchronous contraction. CRT aims to resynchronize contraction by pacing both ventricles simultaneously. Randomized controlled trials found CRT improves symptoms, exercise capacity, and survival in patients with low ejection fraction and wide QRS. Guidelines recommend CRT for class III/IV heart failure patients with LBBB morphology and QRS >120ms. Some evidence also supports benefit in milder heart failure. Response can vary and not all patients respond equally.


![COMPANION Subgroup Analysis COMPANION study 1 year duration Randomized CRT-P, CRT-D, OMT in 2:2:1 ratio Subgroup analysis LBBB: 215 OMT and 426 CRT-P patients Other includes RBBB and IVCD: 93 OMT and 190 CRT-P patients LBBB Other Favors CRT Bristow M, et al. N Engl J Med 2004; 350:2140-50. [COMPANION sponsored by Guidant]](https://image.slidesharecdn.com/cardiacresynchronization-120229215328-phpapp02/85/Cardiac-resynchronization-14-320.jpg)
![Sub-analyses of RBBB from Other Randomized Controlled Studies MIRACLE 1 313 patients with LBBB, 43 with RBBB With CRT, RBBB patients improved NYHA class compared to control With CRT, RBBB patients’ improvements in exercise time and peak VO 2 did not reach statistical significance Pooled data from MIRACLE and Contak CD studies 2 61 patients with RBBB (34 CRT, 27 Control) CRT improved NYHA Class compared to control Trends toward improved QoL, 6 minute walk distance, norepinephrine (NE) with CRT compared to baseline, but with no difference compared to control 1. Aranda J, et al. Clin Cardiol 2004;27: 678–82. [MIRACLE was sponsored by Medtronic] 2. Egoavil CA, et al. Heart Rhythm 2005;2:611–615. [Contak CD was sponsored by Guidant]](https://image.slidesharecdn.com/cardiacresynchronization-120229215328-phpapp02/85/Cardiac-resynchronization-15-320.jpg)

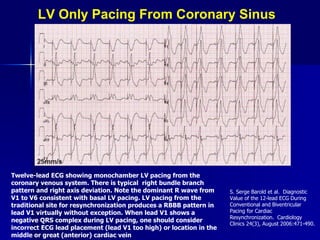
![Q Wave in I Georger and colleagues observed a q wave in lead I in 17 of 18 patients during biventricular pacing As indicated previously, a q wave in lead I during uncomplicated RV apical pacing is rare, and these workers observed it in only one patient. Loss of the q wave in lead I was 100% predictive of loss of LV capture. It therefore appears that analysis of the Q/q wave or a QS complex in lead I may be a reliable way to assess LV capture during biventricular pacing. Georger F, et al. Specific electrocardiographic patterns may assess left ventricular capture during biventricular pacing. PACE ; 25 (2002), p. 56 [abstract].](https://image.slidesharecdn.com/cardiacresynchronization-120229215328-phpapp02/85/Cardiac-resynchronization-45-320.jpg)



































































