


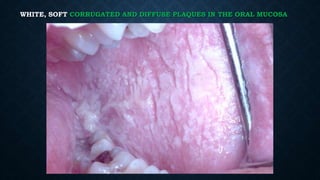




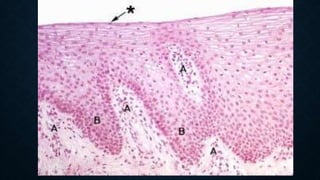









White sponge nevus is a rare, autosomal-dominant disorder affecting the oral mucosa, first described in 1909, characterized by soft, white, corrugated plaques that are painless and non-scrapable. It typically presents in early childhood, has a prevalence of less than 1 in 200,000, and is associated with genetic factors and mutations in keratin genes. Differential diagnoses include various conditions such as oral lichen planus and leukoplakia, with treatment options including antibiotics and antifungals to manage superimposed infections.