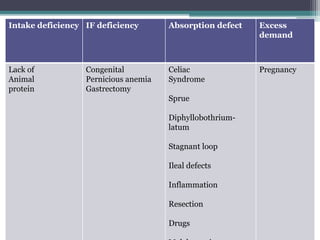
Vitamin B12 is the last vitamin discovered and is essential for nervous system and blood cell formation. Deficiency is common, affecting over 50% of women and 30% of men. It is produced by bacteria and contains cobalt. Absorption requires intrinsic factor in the stomach and occurs in the ileum. Deficiency can result from lack of intake, intrinsic factor deficiency causing pernicious anemia, or absorption issues from diseases or drugs impairing absorption. Diagnosis involves blood tests and the Schilling test to identify the cause of deficiency. Treatment involves B12 injections or high dose oral supplementation.









![Magnesium [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/magnesiumautosaved-140828145928-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


















![VITAMIN B12[CYNACOBALAMIN][COBALAMIN],SOURCES OFVITAMIN B12,VITAMIN B12 DEFIC...](https://cdn.slidesharecdn.com/ss_thumbnails/vitaminb12ravisankar-vignanpharmacy-130615121944-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




