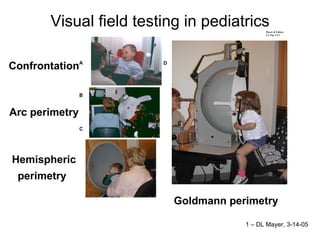
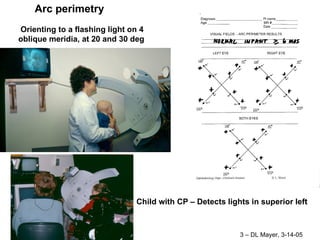
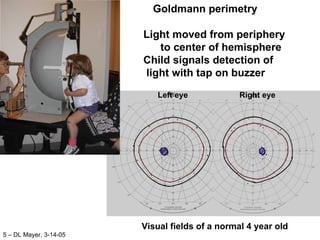
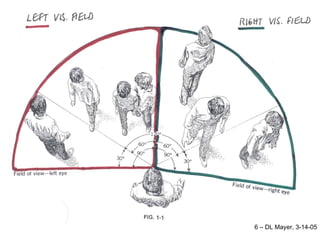
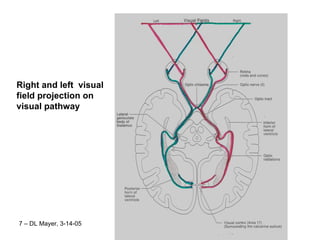
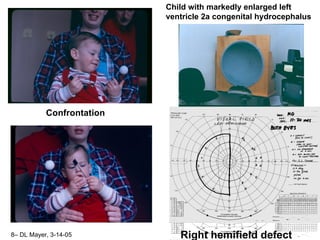
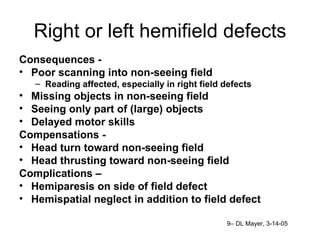
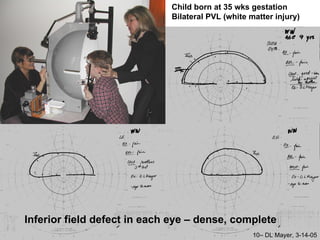
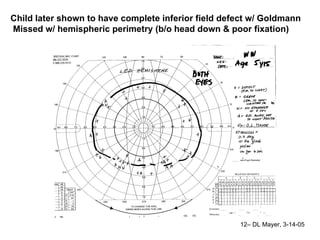
The document discusses different techniques for visual field testing in pediatrics, including confrontation arc perimetry, hemispheric perimetry, and Goldmann perimetry. It provides examples of visual field defects seen in different pediatric patients, such as right or left hemifield defects, and inferior field defects. The document also outlines consequences of visual field defects, compensation strategies, and recommendations for children with major visual field defects.