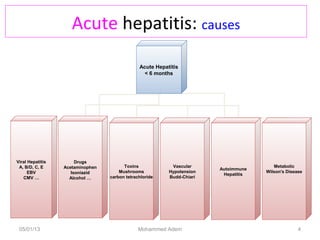
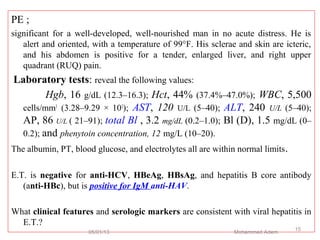
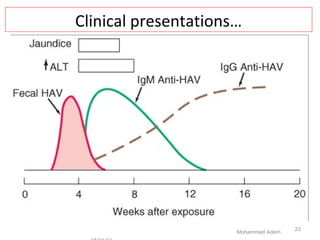
Viral Hepatitis can be either acute or chronic. Acute Hepatitis A virus (HAV) causes inflammation of the liver that is usually self-limiting and does not result in chronic infection. It is commonly spread through the fecal-oral route or contaminated food/water. Clinical presentation involves nonspecific symptoms initially, followed by jaundice. Treatment is supportive and recovery is expected within 1-2 months.