1. Acute viral hepatitis can be caused by hepatitis A, B, C, D, or E viruses. It presents with inflammation of the liver and symptoms like jaundice, nausea, and fatigue that typically resolve within 6 months.
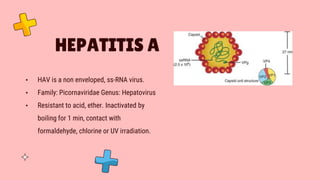
2. Hepatitis A virus is transmitted via the fecal-oral route or contaminated food/water. It causes a self-limiting disease with most children being asymptomatic and 80% of adults experiencing symptoms.
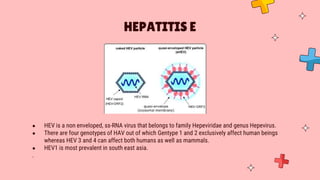
3. Hepatitis E virus is transmitted similarly and can also be zoonotic. It occasionally causes fulminant hepatic failure in pregnant women, those with pre-existing liver disease, and malnourished individuals. Chronic infection is seen in immunocompromised patients






























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



