Downloaded 176 times



![Cardiovascular System:
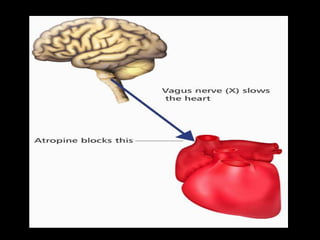
• Dominant effect:Tachycardia by blocking vagal effects
on M2 Ach receptors on SA node.
• But HR often decreases transiently with average
clinical doses[0.4-0.6mg] - due to blockade of inhibitory
presynaptic M1 acetylcholine receptors on vagal nerve
endings - increased acetylcholine release
• HR slowing rarely marked (4-8 beats/min)and
usually absent after rapid I.V. injection.
• Influence on HR - most noticeable in young adults
as vagal tone is considerable.
• In infants and elderly-large doses fail to cause
tachycardia.
• It also shortens AV conduction time and functional
refractory period of AV node.](https://image.slidesharecdn.com/vinayakatropineglyco-150118021024-conversion-gate02/85/Vinayak-atropine-glyco-15-320.jpg)
![CLINICAL USES
PREOPERATIVE MEDICATION:
Historically,atropine was given i.m. before induction to protect the
heart from vagal reflexes and to prevent excess salivary secretion.
Currently used anesthetic agents are not predictably associated with
these effects hence not mandatory to include an anticholinergic in
preop medication.
Hence most likely goal is to produce sedation or antisialogogue
effect.
DOSAGE:
Adults:
i.v./i.m.-0.4-1mg
Orally-0.4-0.6mg every 4-6 hrs
Children:
i.v.-10-20mcg/kg[min 0.1mg]
Oral-30 mcg/kg every 4-6hrs.](https://image.slidesharecdn.com/vinayakatropineglyco-150118021024-conversion-gate02/85/Vinayak-atropine-glyco-21-320.jpg)
![REVERSAL OF NEUROMUSCULAR
BLOCKADE
Antagonism of Nondepolarising NM blocking
drugs with an anticholinesterase requires the
use of Atropine to prevent parasympathomimetic
effects of the anticholinesterase.
Depending on the speed of onset of
Anticholinesterase action, Atropine[rapid onset]
or glycopyrrolate[slow onset] is selected.
DOSAGE:0.015mg/kg with
neostigmine[i.v.0.05mg/kg] or
edrophonium[i.v.0.5-1mg/kg]](https://image.slidesharecdn.com/vinayakatropineglyco-150118021024-conversion-gate02/85/Vinayak-atropine-glyco-23-320.jpg)
![BRONCHODILATION
• Atropine,1-2mg/kg diluted in 3-5ml NS can be
administered via nebuliser to treat bronchial
asthma.
OTHER USES OF ANTICHOLINERGICS :
• Biliary and Ureteric smooth muscle relaxation.
• Mydriasis and cycloplegia
• Antagonism of gastric H+ ion secretion.
• Management of Parkinson’s disease and
treating extrapyramidal side effects of
antidopaminergic drugs.
• Treatment of hiccups [atropine 0.5 mgi.v.
terminates hiccups following LMA insertion].](https://image.slidesharecdn.com/vinayakatropineglyco-150118021024-conversion-gate02/85/Vinayak-atropine-glyco-24-320.jpg)
![CLINICAL USES
PREOPERATIVE MEDICATION
It is now preferred to atropine as:
• No CNS cognitive effects.
As per BJA 1987[vol.59,966-969],no cognitive changes
after surgery were seen with glycopyrrolate as preop
medication,while with atropine significant short term
memory deficit was seen.
• CVS effects are less pronounced and for shorter
duration than atropine,hence more stable
hemodynamically.
Dosage:
• i.v./i.m./s.c.:0.1-0.2mg[4-6mcg/kg]
• Orally:50 mcg[1mcg/kg].](https://image.slidesharecdn.com/vinayakatropineglyco-150118021024-conversion-gate02/85/Vinayak-atropine-glyco-31-320.jpg)
![REVERSAL OF NEUROMUSCULAR
BLOCKADE
• Glycopyrrolate is used when slow onset[2-3min]
of action is desired,as with neostigmine.
• Impairment of parasympathetic nervous system
control of HR is of shorter duration than
atropine,hence preferable for patients at risk for
CVS complications like cardiac dysrhythmias in
response to myocardial ischemia and decreased
survival after MI.
Dosage:
• 0.01mg/kg with iv neostigmine 0.05mg/kg[0.2mg
for each 1mg of neostigmine] or iv
pyridostigmine 0.25mg/kg.](https://image.slidesharecdn.com/vinayakatropineglyco-150118021024-conversion-gate02/85/Vinayak-atropine-glyco-32-320.jpg)
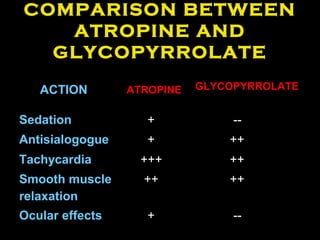


This document provides information about atropine and glycopyrrolate, including their structure, mechanisms of action, pharmacokinetics, clinical uses, and comparisons. Atropine is a competitive muscarinic receptor antagonist derived from plants. It has central nervous system and cardiovascular effects. Glycopyrrolate is a quaternary ammonium anticholinergic that does not cross the blood brain barrier, so it has fewer central effects. Both drugs are used preoperatively and to reverse neuromuscular blockade. Glycopyrrolate is preferred to atropine for premedication due to its more stable hemodynamic profile and lack of cognitive effects.



































































