1. Valvular heart disorders involve abnormalities of the valves that regulate blood flow through the heart. The main types are mitral valve prolapse, mitral stenosis, and mitral regurgitation.
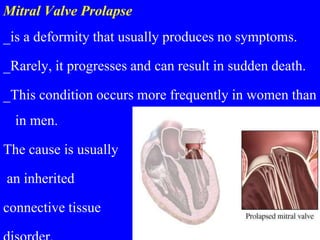
2. Mitral valve prolapse involves a portion of the mitral valve bulging back into the left atrium. Mitral stenosis is a narrowing of the mitral valve that obstructs blood flow. Mitral regurgitation allows blood to flow back from the left ventricle to the left atrium.
3. Nursing management of valvular disorders focuses on patient education, medication administration, monitoring for symptoms, and supporting patients through valve repair or replacement procedures.