Downloaded 110 times


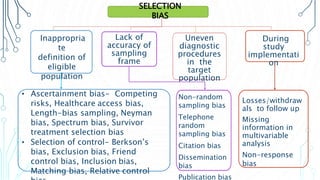

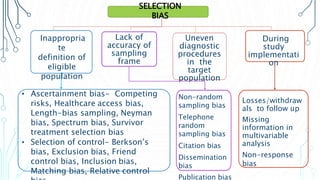
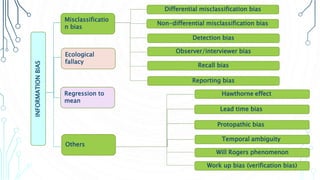
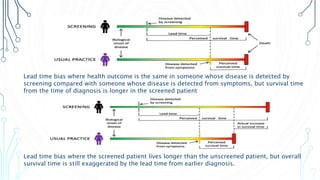
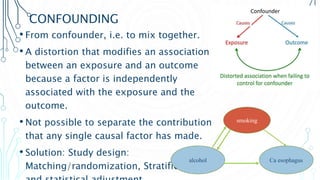
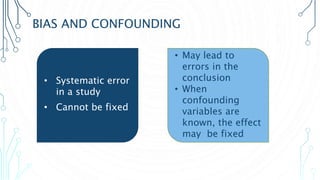




The document discusses the validity and types of biases in epidemiological studies, emphasizing the importance of examining study design, data collection, and analysis methods. It categorizes biases into selection, information, and confounding biases, providing examples and potential solutions to mitigate their effects. Additionally, it explores various specific biases, such as recall bias, observer bias, and lead time bias, which can distort findings and impact the conclusions drawn from research.






















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)












