Downloaded 102 times
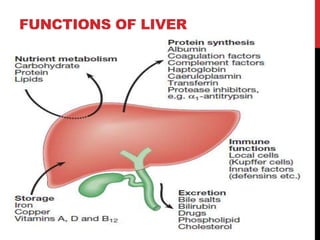
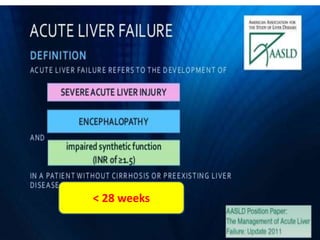
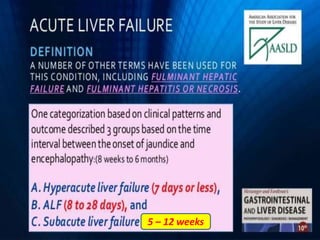
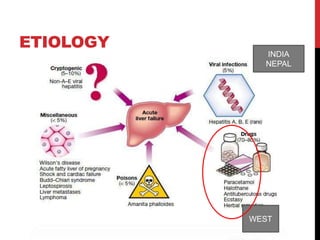
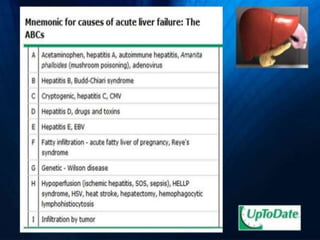
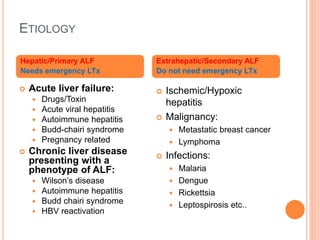
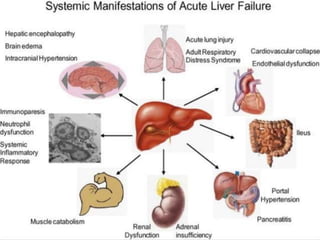
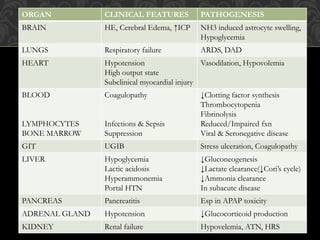
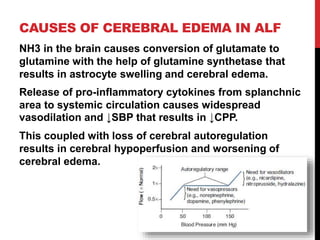
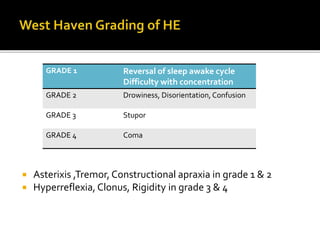
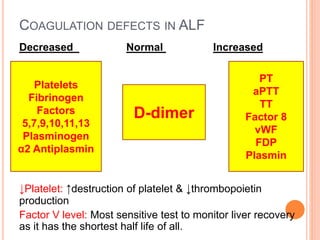
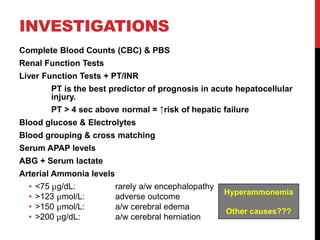
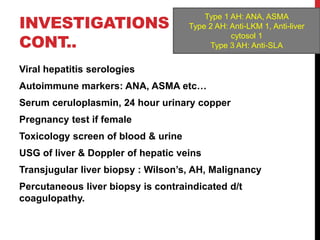
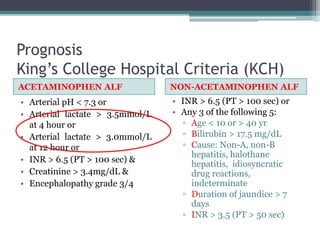
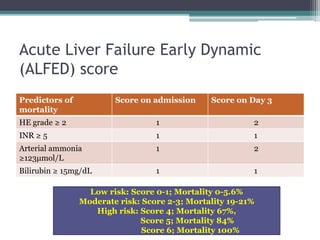

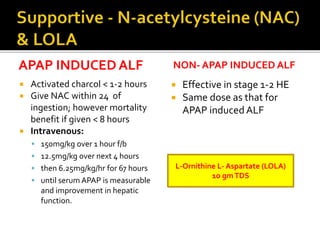
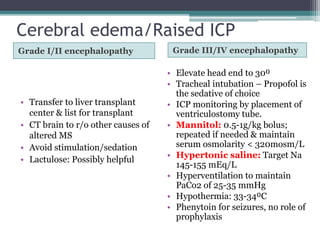
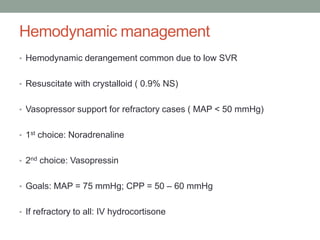
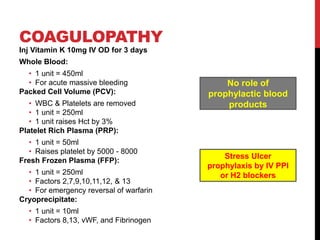
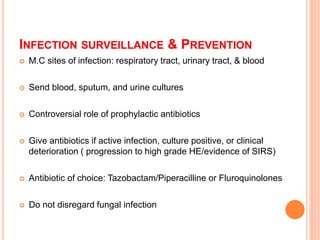



This document provides information about acute liver failure (ALF), including its definition, etiology, pathophysiology, clinical features, investigations, prognosis, and management. ALF is characterized by severe liver injury and encephalopathy within 8 weeks without pre-existing liver disease. Common causes include drugs/toxins, viral hepatitis, and autoimmune conditions. In ALF, liver cells die rapidly, impairing ammonia clearance and coagulation factor production, which can lead to cerebral edema, coagulopathy, and multi-organ failure without transplantation. Prognosis is assessed using tools like KCH or ALFED scores. Management involves supportive care, treating the underlying cause, and considering transplantation for eligible patients.