Downloaded 78 times

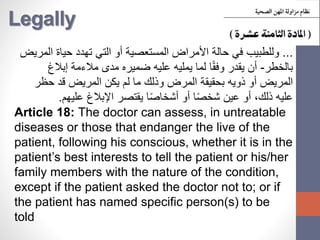
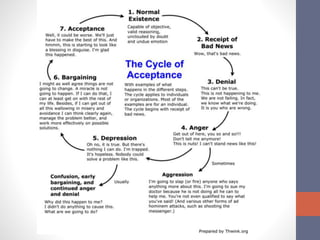
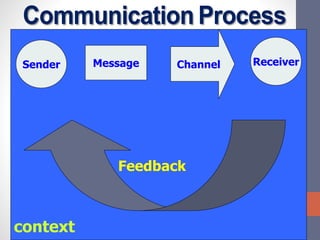
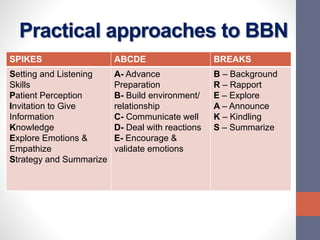
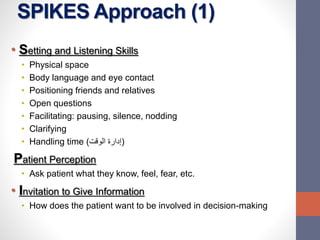
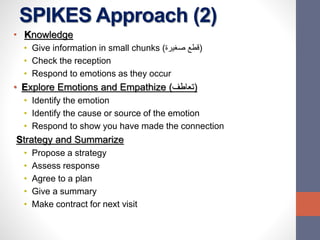
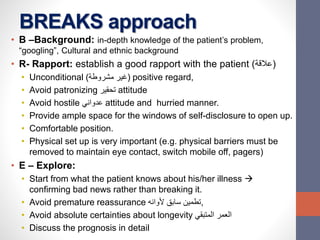


The document discusses the ethical principles and practical steps involved in breaking bad news (BBN) to patients. It outlines the importance of truth-telling, identifying bad news situations, and describes systematic approaches like the SPIKES and ABCDE protocols for delivering difficult information. Additionally, it addresses patient reactions to bad news and provides guidelines on effective communication strategies in these sensitive scenarios.

![[Behav. sci] breaking bad news by SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/8kazuikbs0wrpvxfrejb-signature-413e8c33574c21294a6dc95e37151f54f981375d6b0f4695b85074f597ea60c2-poli-150813085608-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)













































![07.BREAKING_BAD_NEWS[1].pptx this is partcular](https://cdn.slidesharecdn.com/ss_thumbnails/07-240919072838-9a18c1d5-thumbnail.jpg?width=640&height=640&fit=bounds)






















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















