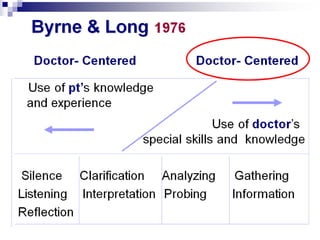
The document discusses various consultation models in family medicine, including traditional disease-focused models and more comprehensive models that emphasize the patient-physician relationship and address psychosocial factors. It then presents Fayza Rayes' comprehensive consultation model, which aims to integrate effective communication skills into the traditional clinical method in a practical way that can be incorporated into daily practice and medical records. The model emphasizes a patient-centered and holistic approach that addresses patient needs beyond just disease management.

















































![AETCOM [ATTITUDE,ETHICS & COMMUNICATION IN MEDICAL EDUCATION] EDUCATION](https://cdn.slidesharecdn.com/ss_thumbnails/aetconnewpppt-200525080043-thumbnail.jpg?width=640&height=640&fit=bounds)
















































![Introduction FM2 [2014]](https://cdn.slidesharecdn.com/ss_thumbnails/2014introductionfmii-140218165323-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Introduction FM3 [2014]](https://cdn.slidesharecdn.com/ss_thumbnails/2014introductionfmiii-140130091159-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)































