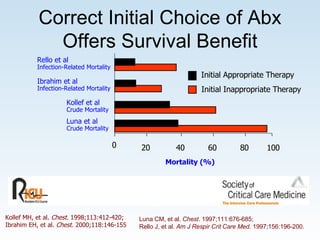
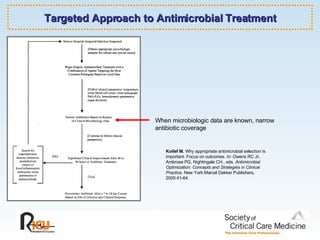
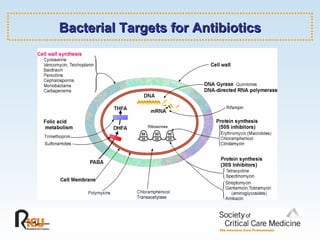
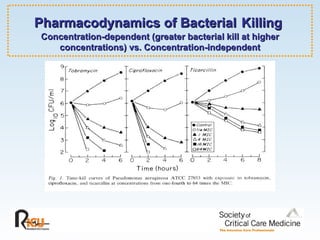
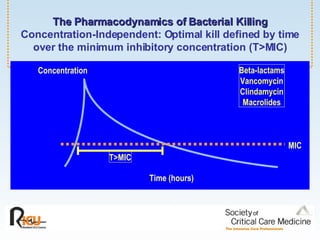
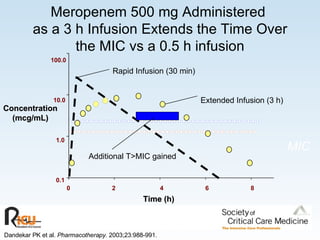
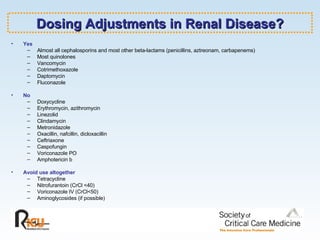
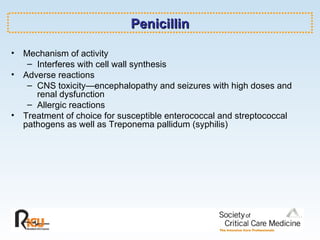
The document discusses principles of treating infectious illnesses in critical care, with a focus on antibiotic resistance and choice of antibiotics. It covers several topics: the impact of antibiotic use on resistance; choosing initial antibiotics and tailoring treatment based on culture results; applying pharmacology and pharmacodynamics to optimize bacterial killing; and reviewing guidelines for specific infections. It also provides an overview of antibiotic classes, mechanisms of action, considerations for dosing in renal impairment, and highlights specific agents like penicillins, cephalosporins, and vancomycin.