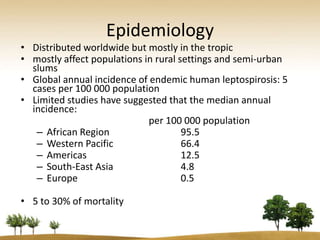
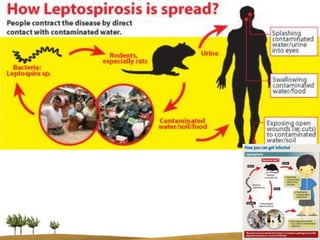
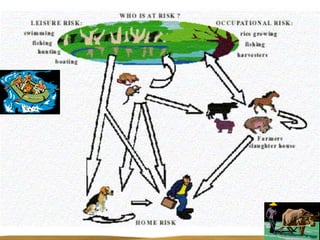
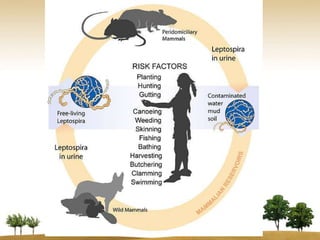

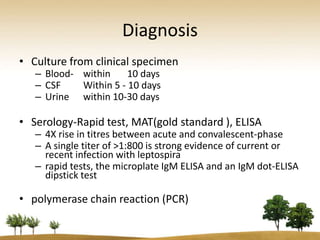
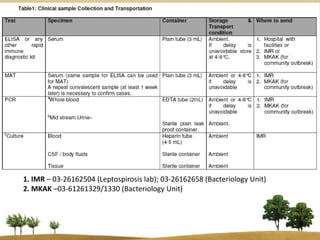
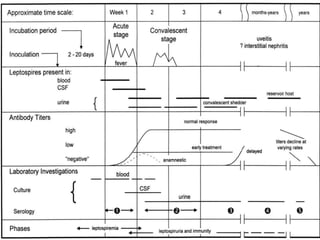
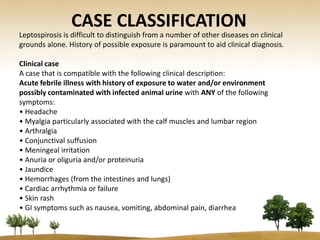
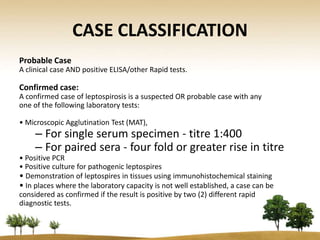

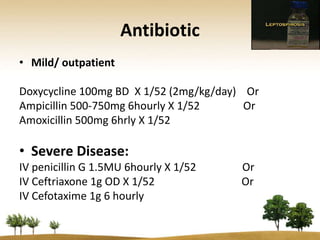
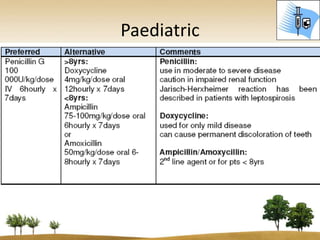
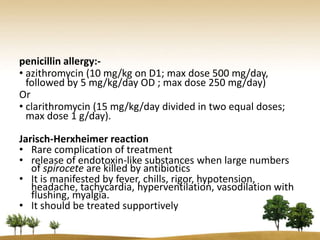
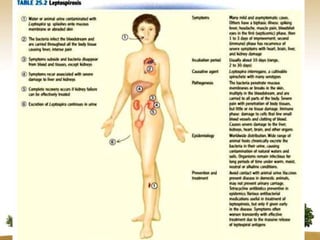
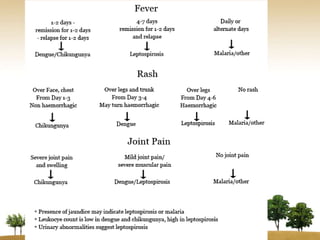
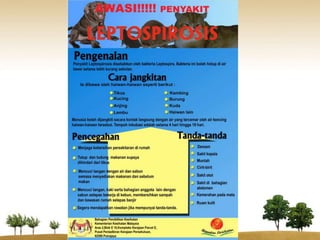

Leptospirosis is a bacterial disease caused by Leptospira interrogans that is distributed worldwide but mostly affects populations in rural and semi-urban areas. It is transmitted through contact with water or soil contaminated by infected animal urine. Clinical presentation varies from mild flu-like symptoms to severe disease affecting multiple organs. Diagnosis involves serological tests, culture or PCR. Treatment is with doxycycline or penicillin with supportive care for organ complications. Prevention focuses on rodent control, vaccination of animals, and avoiding contact with contaminated water sources.



































































