Downloaded 521 times

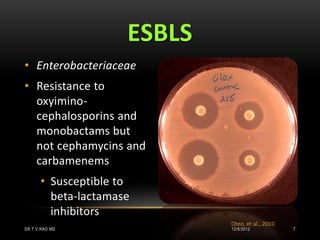
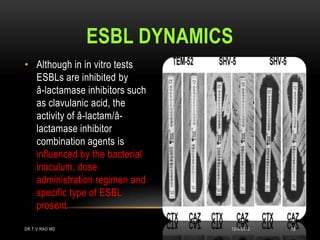







This document discusses drug resistant gram-negative bacteria. It notes that there are currently no new drugs to treat infections from multidrug-resistant gram-negative bacilli such as Acinetobacter baumannii and Pseudomonas aeruginosa. It also discusses extended-spectrum beta-lactamases (ESBLs) which are enzymes produced by bacteria that confer resistance to many beta-lactam antibiotics. The document provides information on detecting and confirming ESBL production in bacteria.































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



