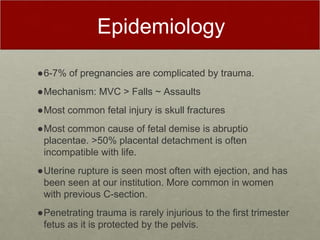
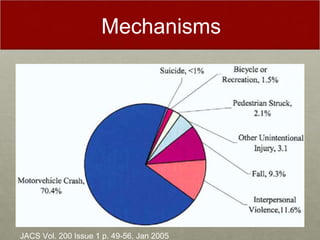
- Trauma is complicated in approximately 6-7% of pregnancies. Common injuries include skull fractures in the fetus from motor vehicle collisions and placental abruption.
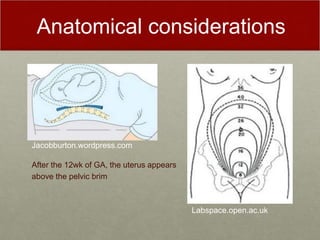
- After 12 weeks of gestation, the uterus rises above the pelvis and is at risk of direct injury. Penetrating trauma before 12 weeks rarely harms the fetus which is protected in the pelvis.
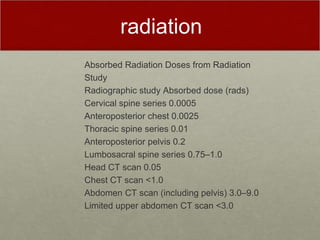
- Radiation exposure should be limited by shielding the uterus, with exposures under 0.1 Gy considered safe. CT scans present the greatest risk and alternative imaging like FAST ultrasound is preferred.
- If the mother arrests, CPR and rapid c-section within 15 minutes may save a viable late-term fetus. Maternal outcomes