This document discusses transfusion medicine and guidelines for blood transfusion therapy. It covers:
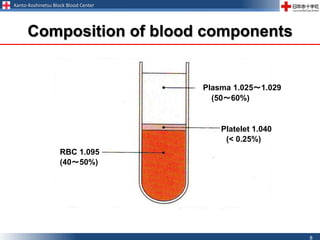
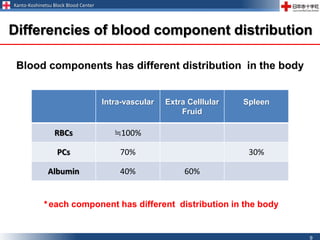
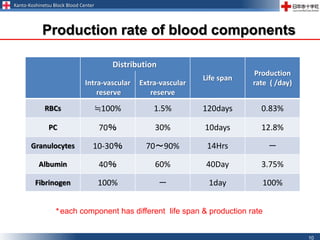
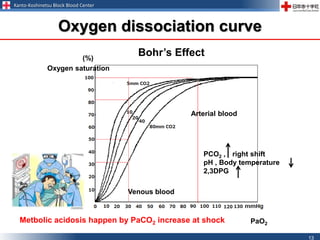
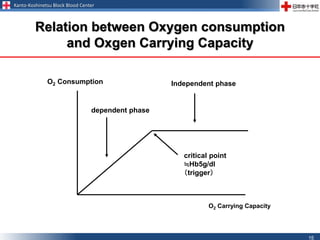
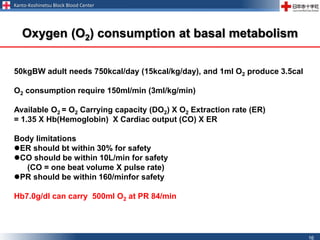
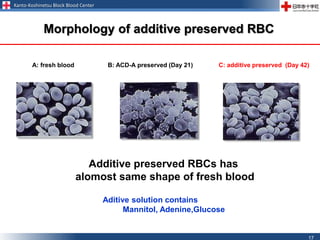
1. The main components transfused (red blood cells, platelets, fresh frozen plasma) and their functions in supplementing oxygen carrying capacity, coagulation factors, and blood volume.
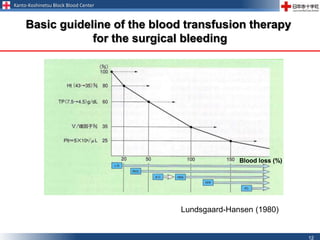
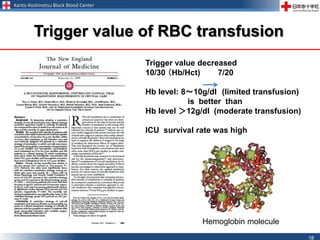
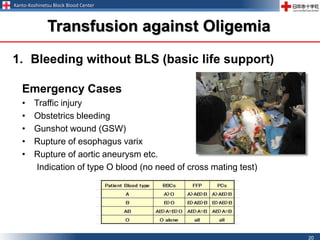
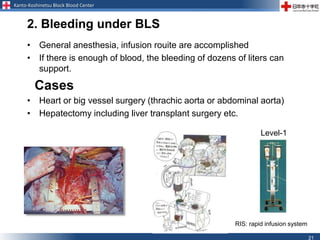
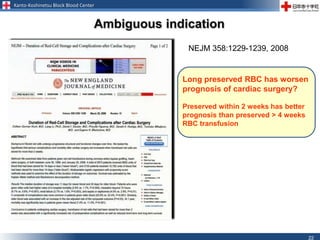
2. Indications for transfusion based on vital signs, blood tests, and patient factors like blood loss levels and prognosis.
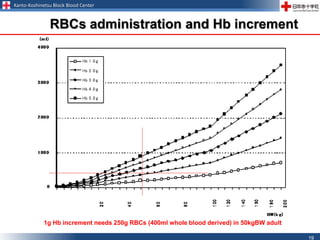
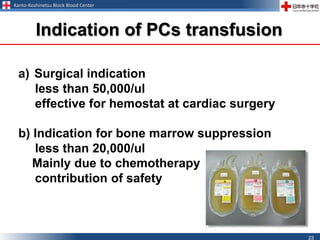
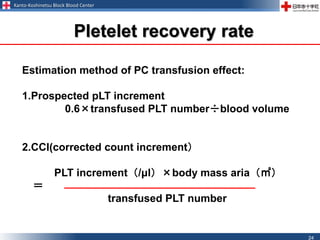
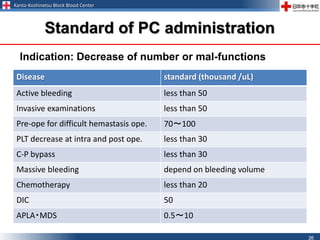
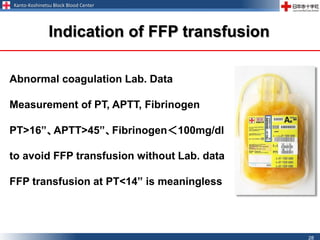
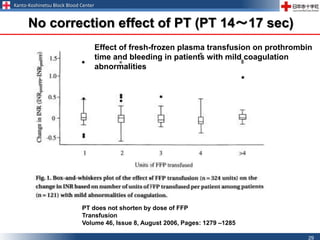
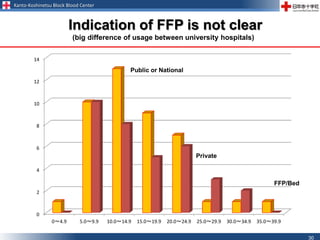
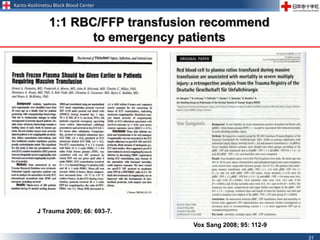
3. Guidelines for transfusing specific components like red blood cells, platelets, and fresh frozen plasma based on concentration thresholds and conditions.
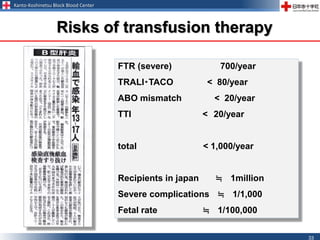
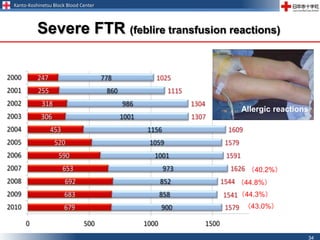
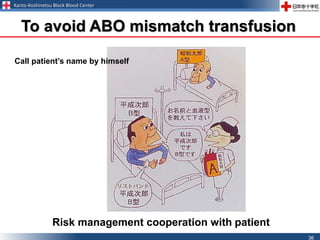
4. Risks of transfusion therapy and the importance of informed consent and risk management.