Download as PDF, PPTX
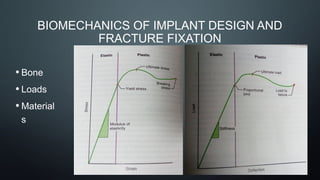

The document provides a comprehensive overview of internal fixators used in fracture treatment, detailing various types and their principles of surgical treatment, including methods of application and biomaterials employed. It discusses the biomechanics of implant design and the characteristics of different fixation methods such as pins, screws, and plates. Additionally, it addresses the complications associated with fixation devices and outlines guidelines for the stabilization of fractures using intramedullary nails.



































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















