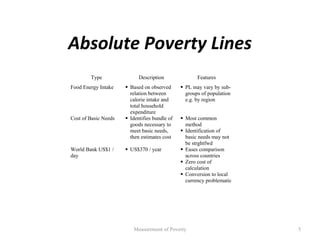
This document discusses concepts and methods for measuring poverty. It notes that while governments collect many statistics on poverty, the data ultimately comes from individual reports that may not be accurate. There are practical concerns in measuring poverty, including defining the poverty line, what unit to measure (individual, household), and what indicators to use. Common methods for setting the poverty line include the food energy intake method and cost of basic needs approach. The food energy intake method sets the poverty line based on the expenditure needed to meet minimum daily calorie requirements. The cost of basic needs approach identifies items in a basic consumption bundle and determines the total cost. Poverty lines may vary by region due to differences in prices and publicly provided goods and services.