Downloaded 57 times

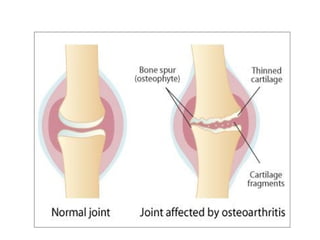
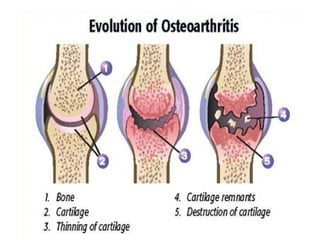
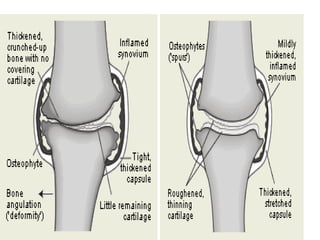
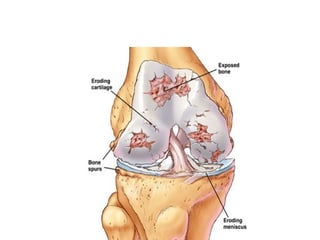
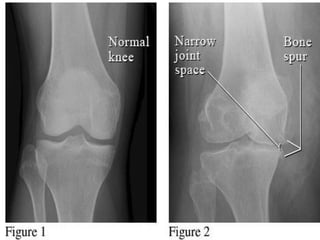
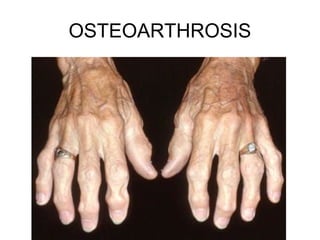
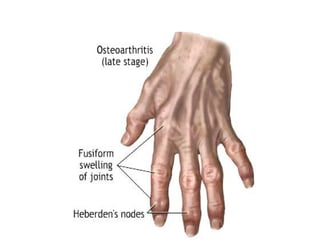
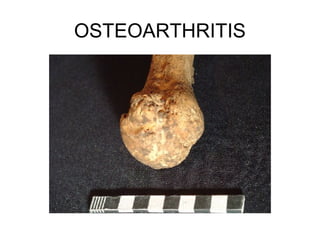
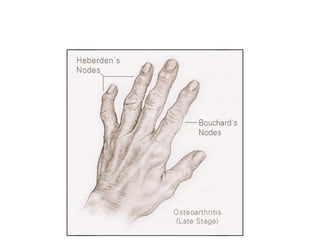
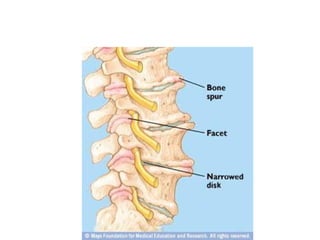

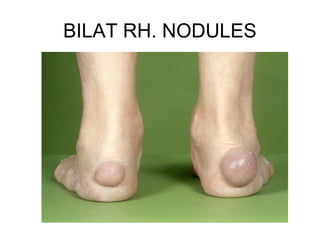
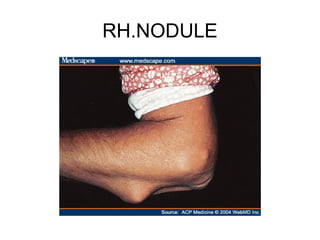
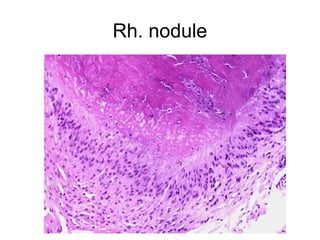
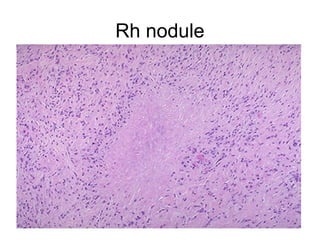



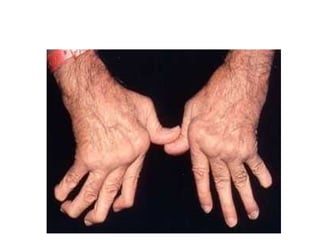


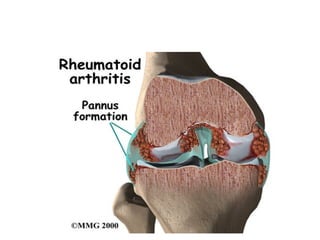



This document summarizes diseases of joints, including normal joint structure and function. It describes osteoarthritis and rheumatoid arthritis in detail. Osteoarthritis is characterized by erosion of articular cartilage in weight-bearing joints. Risk factors include age, mechanical stress, genetics, and bone density. Rheumatoid arthritis is a systemic inflammatory disease that principally attacks synovial joints, causing synovial inflammation and destruction of cartilage and bone. It is mediated by autoimmune reactions involving T cells, B cells, and cytokines like TNF and IL-1.












































![OSTEOARTHRITIS, PATHOLOGY AND MANAGEMENT [Autosaved]_063207.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/osteoarthritispathologyandmanagementautosaved063207-250403031955-f0916f70-thumbnail.jpg?width=640&height=640&fit=bounds)





















