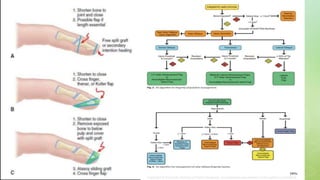
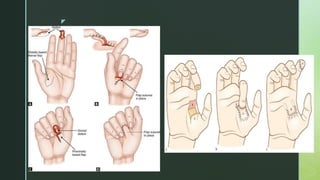
This document provides information on finger tip and soft tissue reconstruction of the hand. It begins with an introduction to finger tip injuries, including common causes. It then discusses the anatomy of the finger tip and classifications of fingertip amputations. Several local flap techniques for reconstructing finger tip defects are described in detail, including composite tip grafts, free pulp grafts, V-Y advancement flaps, homodigital flaps, and cross finger flaps. Goals of management and assessment of injuries are also covered. The document concludes with a discussion of local flaps that can be used for covering defects on the dorsum of the hand.