Download to read offline


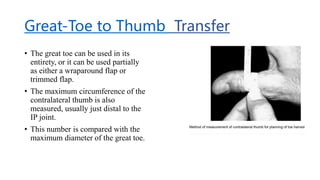









The document discusses toe to thumb transfer as an option for thumb reconstruction. It provides details on: - The anatomy of the toe making it suitable for transfer, including its skeletal structure, tendons, skin, and nerves - The history of toe to thumb transfer, including early experiments and the first microsurgical procedure - Causes of thumb loss that may require reconstruction - Preoperative assessment and considerations for candidates, including smoking cessation - Surgical technique for both hand and toe dissection to prepare the structures for microvascular anastomosis













































































