Downloaded 115 times

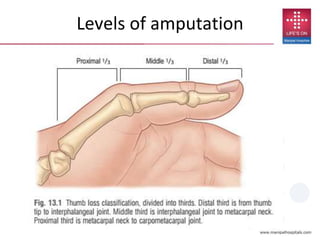
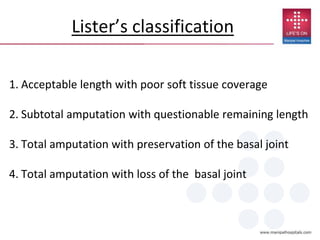

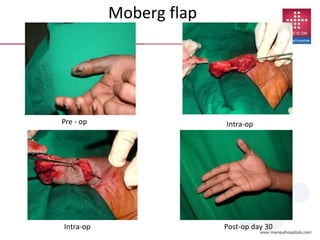
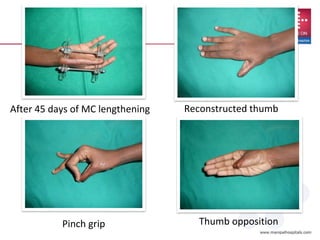
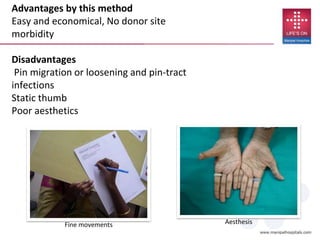


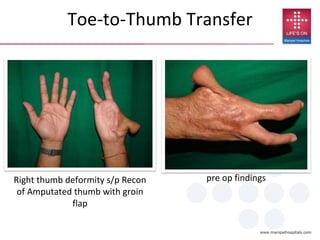

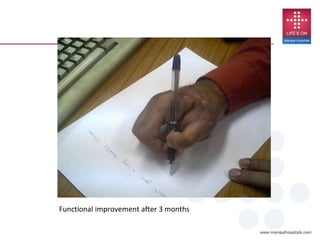
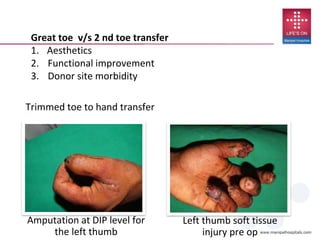
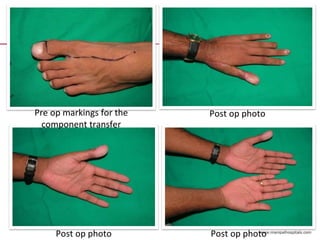

This document discusses reconstruction of the thumb following various types of injuries or amputations. It begins by classifying different levels of thumb amputation and the general goals of reconstruction, which include regaining sensation, stability, strength, mobility and correct posture. Several reconstruction techniques are described for different amputation levels, such as secondary healing, flaps, phalangisation, osteoplastic reconstruction, pollicization, and toe transfers. Factors to consider for the choice of reconstruction include the level of amputation, remaining joints and digits, soft tissue coverage, and patient expectations and functional needs. The conclusion emphasizes that the best results are obtained with replantation when possible and tailoring the approach to the individual patient's post-tra