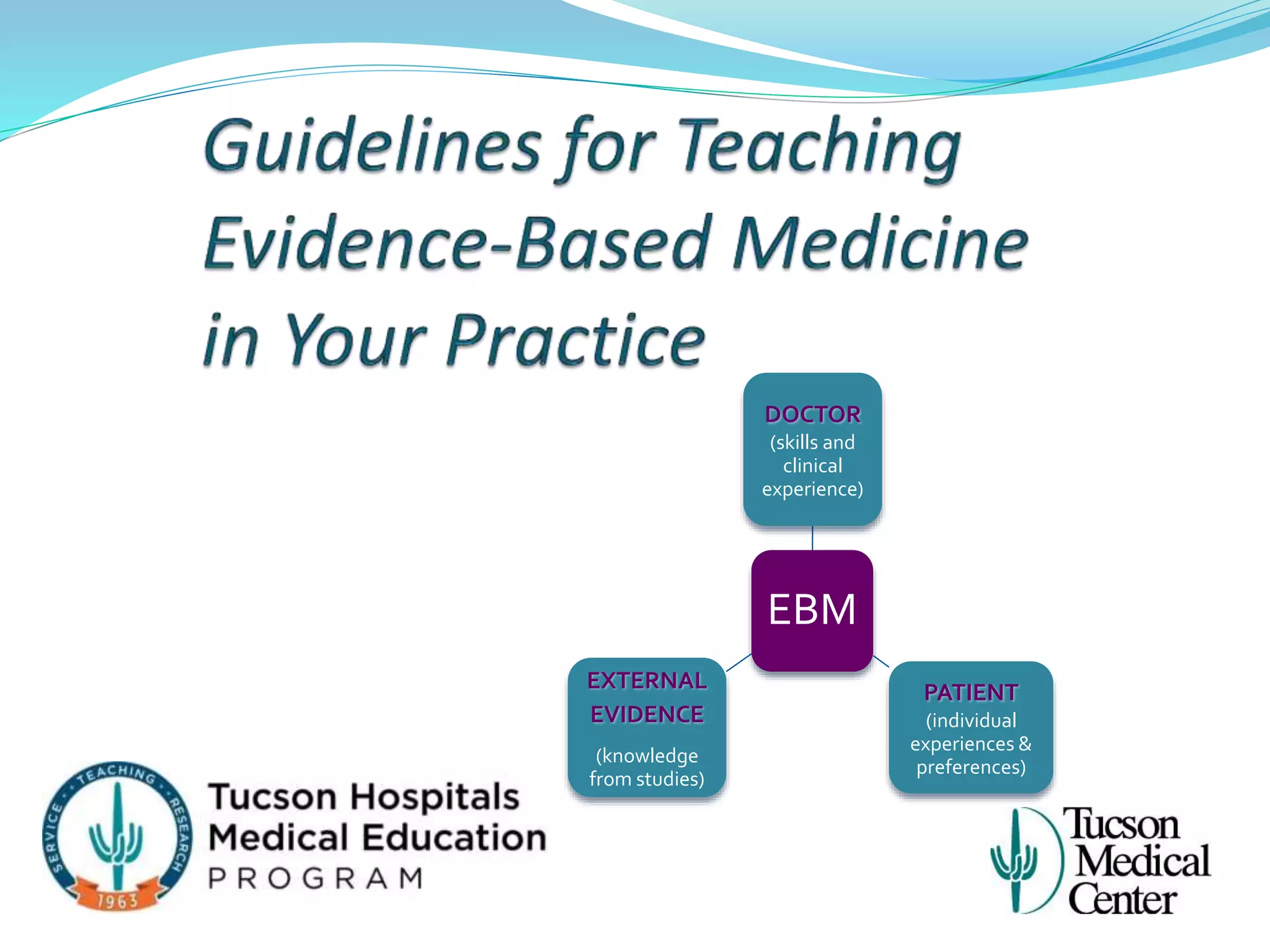
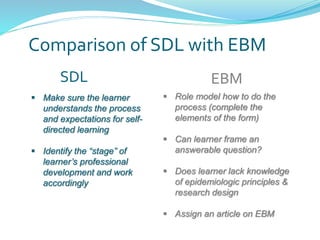
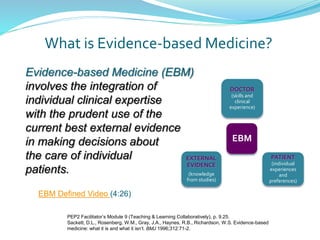
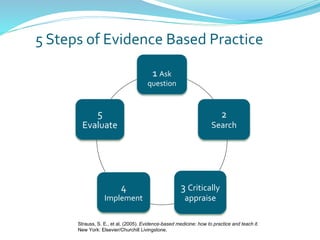
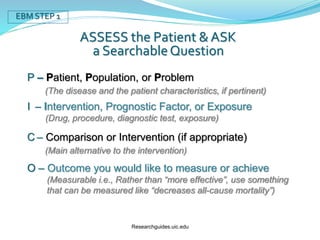
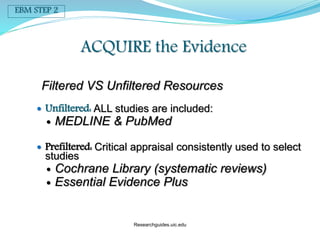
Ryan, a first-year resident, lacks depth in his clinical presentations and relies solely on UpToDate without referencing appropriate medical literature. Dr. Waters encourages Ryan to be more self-directed by following the process of evidence-based medicine (EBM). EBM involves integrating individual clinical expertise with the best external evidence from studies. Dr. Waters can role model EBM for Ryan by completing self-directed learning activities that include formulating answerable clinical questions, efficiently searching medical literature, and critically appraising evidence. Nonadherence to practice guidelines is a major barrier to successfully applying EBM.











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









