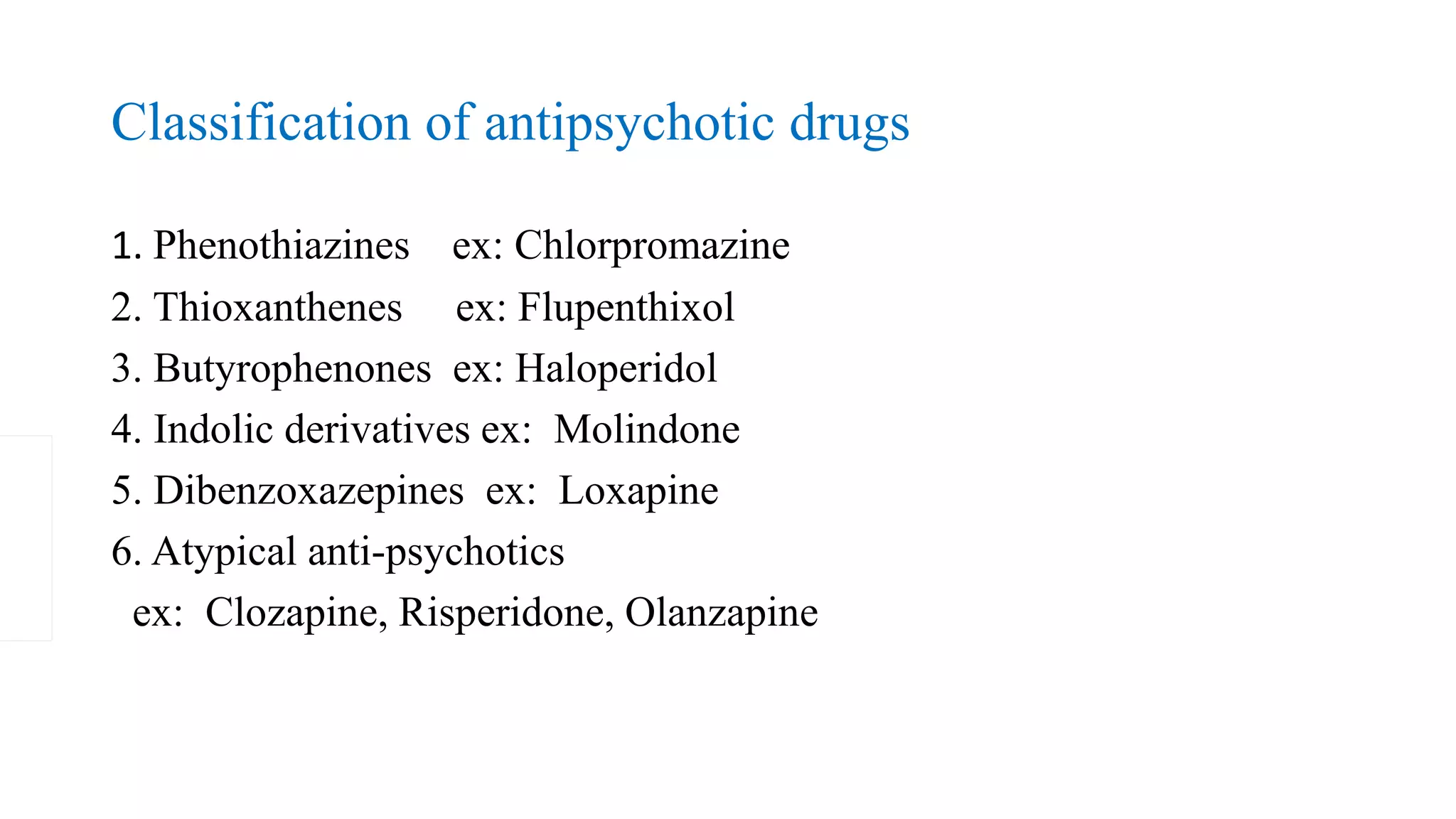
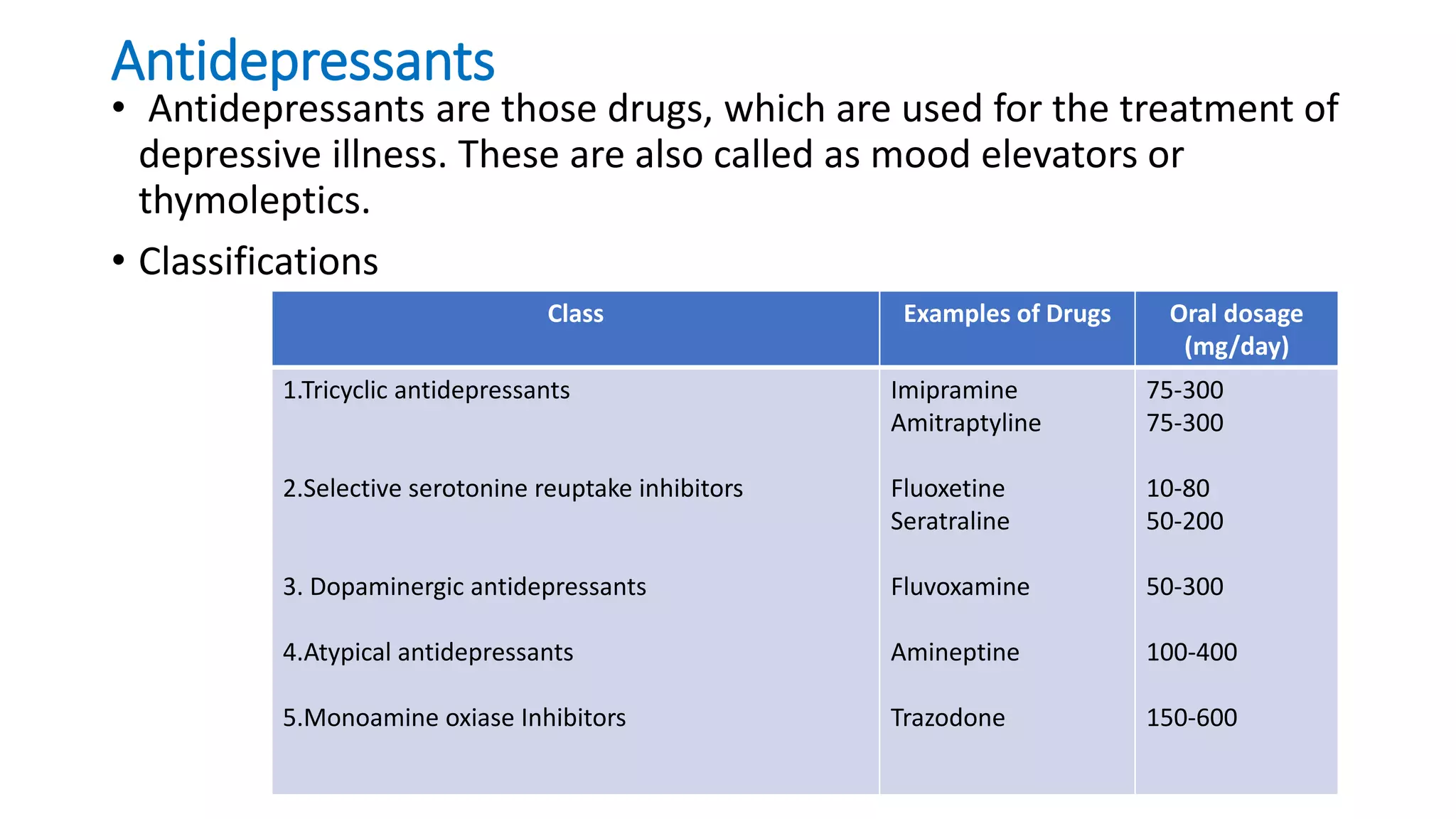
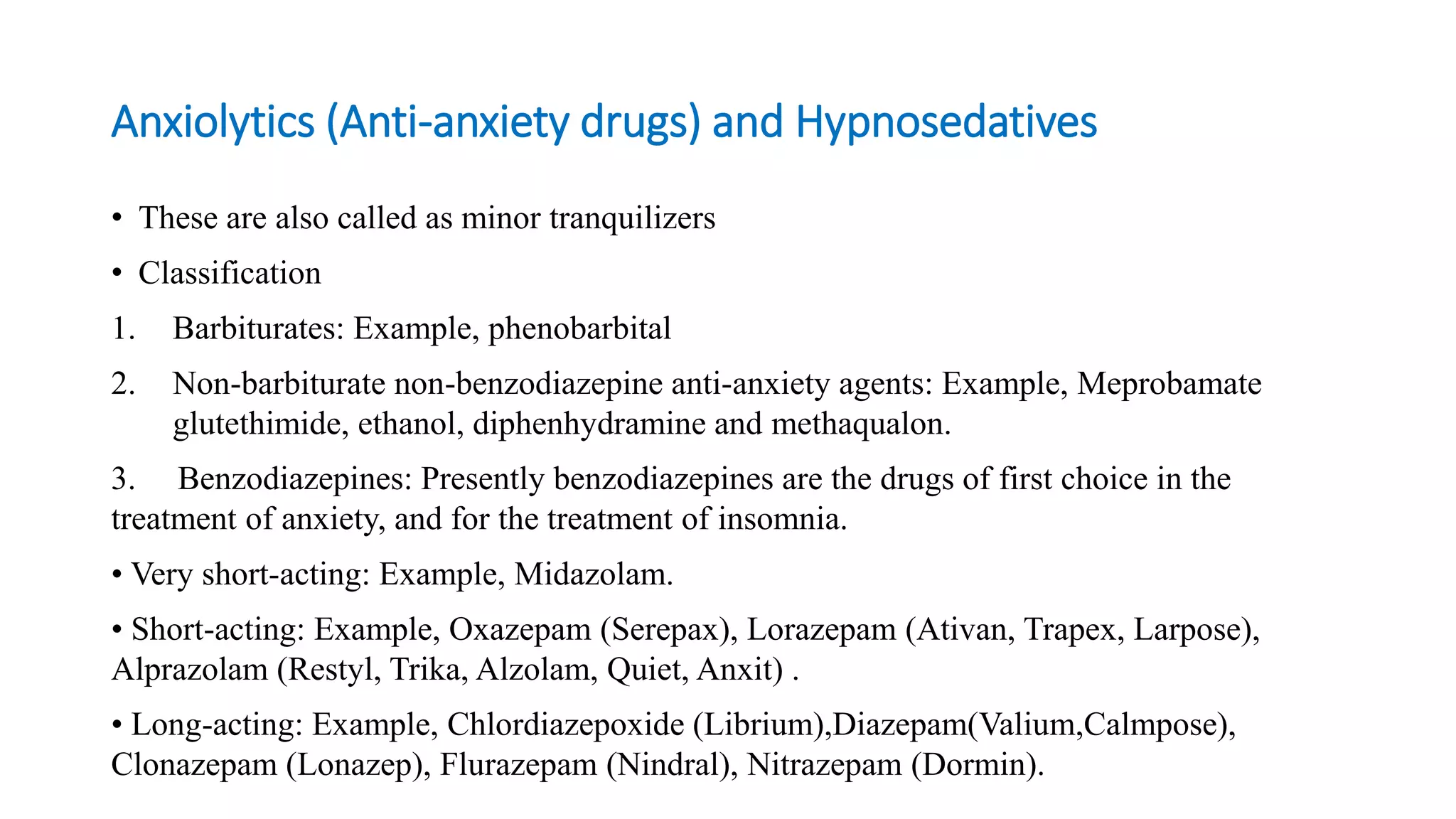
Therapeutic modalities in psychiatry include somatic (physical) therapies like psychopharmacology, electroconvulsive therapy, and psychosurgery. Psychological therapies include various counseling approaches. Milieu therapy aims to provide a supportive environment, while therapeutic communities are highly structured treatment programs. Activity therapies use recreational and occupational activities. Common psychotropic medications include antipsychotics, antidepressants, mood stabilizers, anxiolytics, and drugs used in child psychiatry. Electroconvulsive therapy is used to treat severe depression, catatonia, and psychosis.