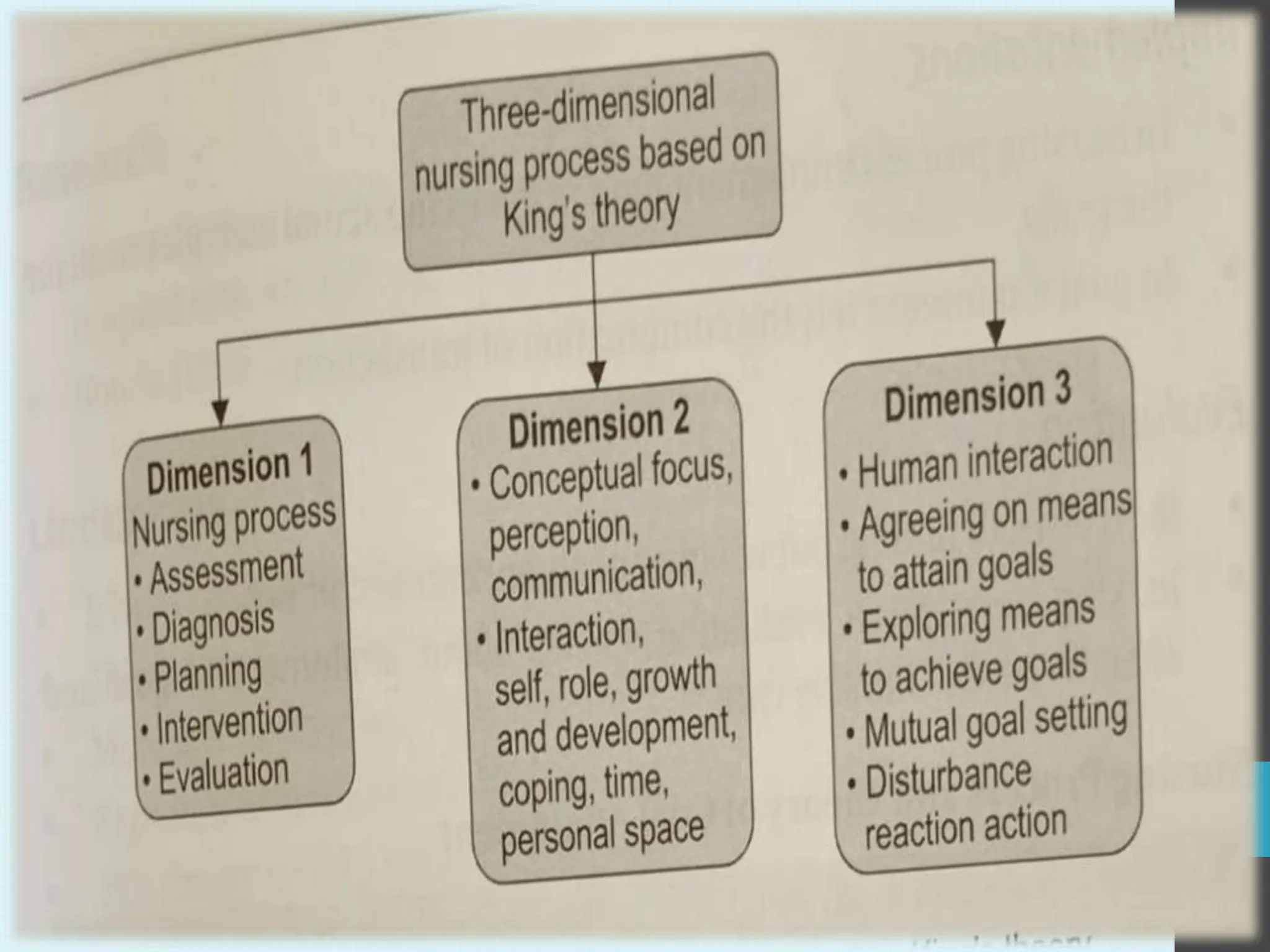
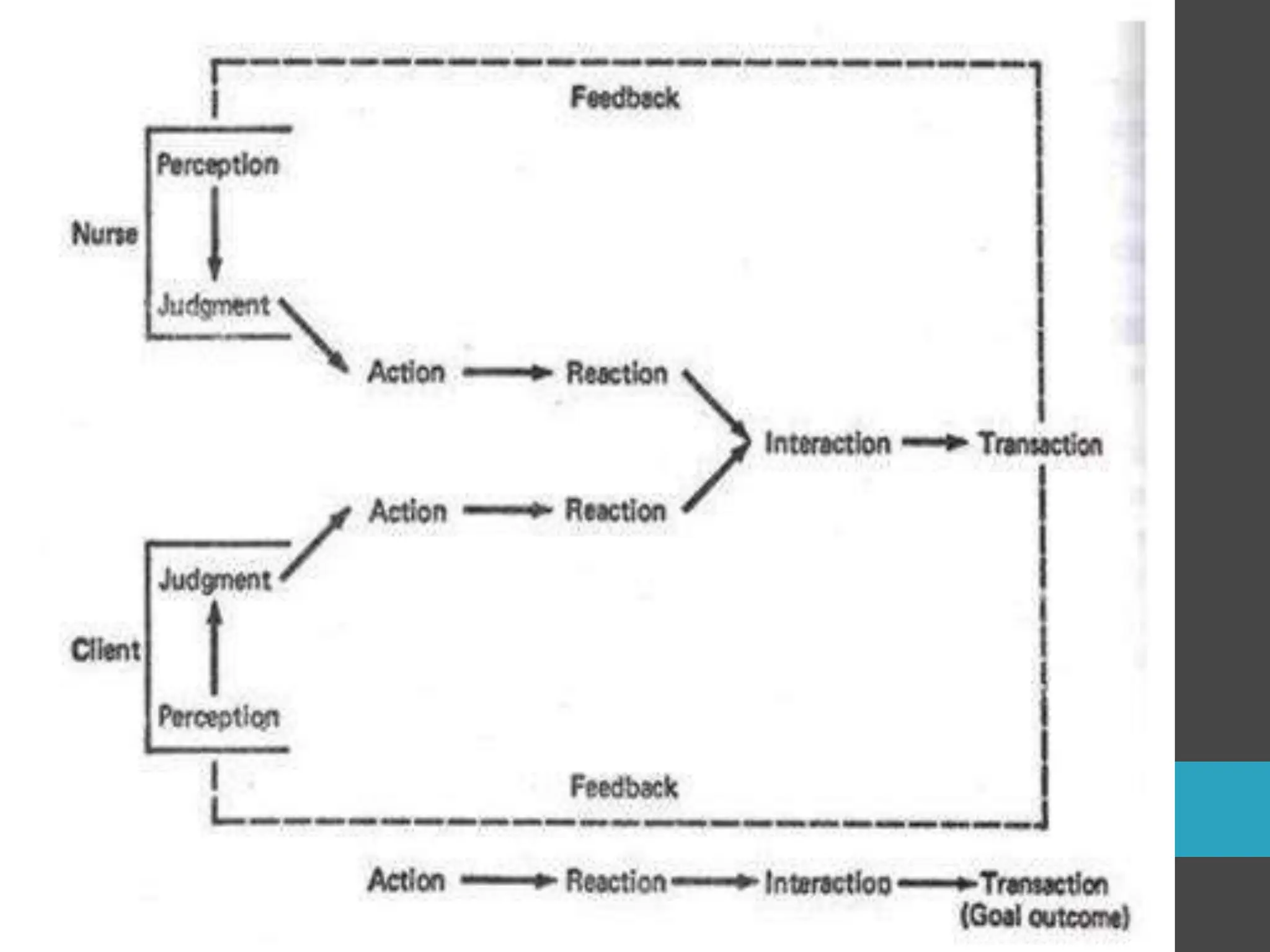
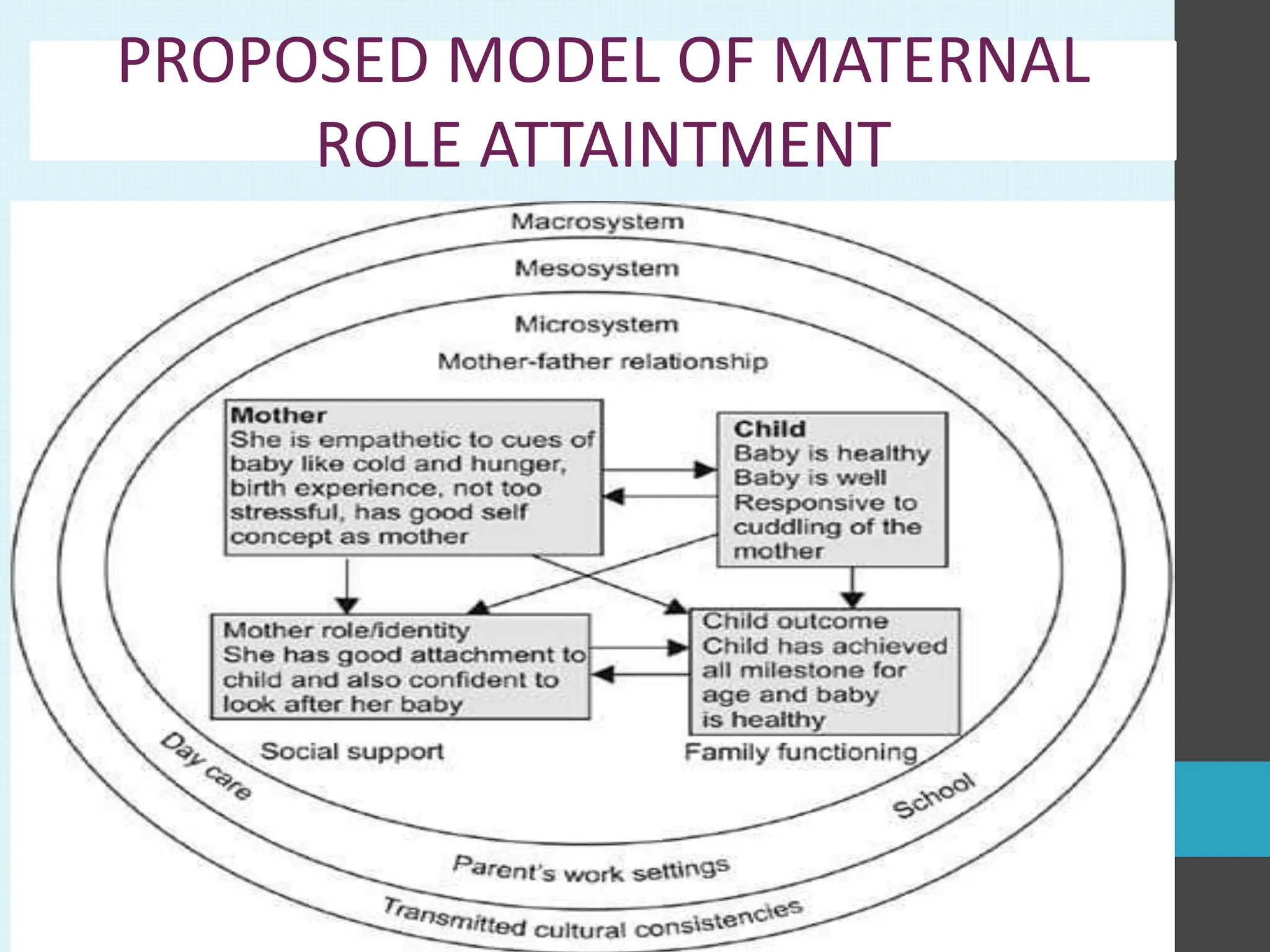
The document discusses various theories related to midwifery practice, emphasizing King’s Goal Attainment Theory and Mercer’s Maternal Role Attainment Theory. King’s theory revolves around the dynamic nurse-client interaction aimed at achieving health care goals, while Mercer’s theory outlines the developmental process of mothers bonding with their infants and the factors influencing maternal identity. It also highlights the importance of social support, family dynamics, and the interaction between maternal and infant characteristics in defining successful maternal role attainment.






























































































































![Imo king [Autosaved].pptx11111111111111theorryytt](https://cdn.slidesharecdn.com/ss_thumbnails/imokingautosaved-250127083514-4d629a1b-thumbnail.jpg?width=640&height=640&fit=bounds)




















































