Downloaded 155 times

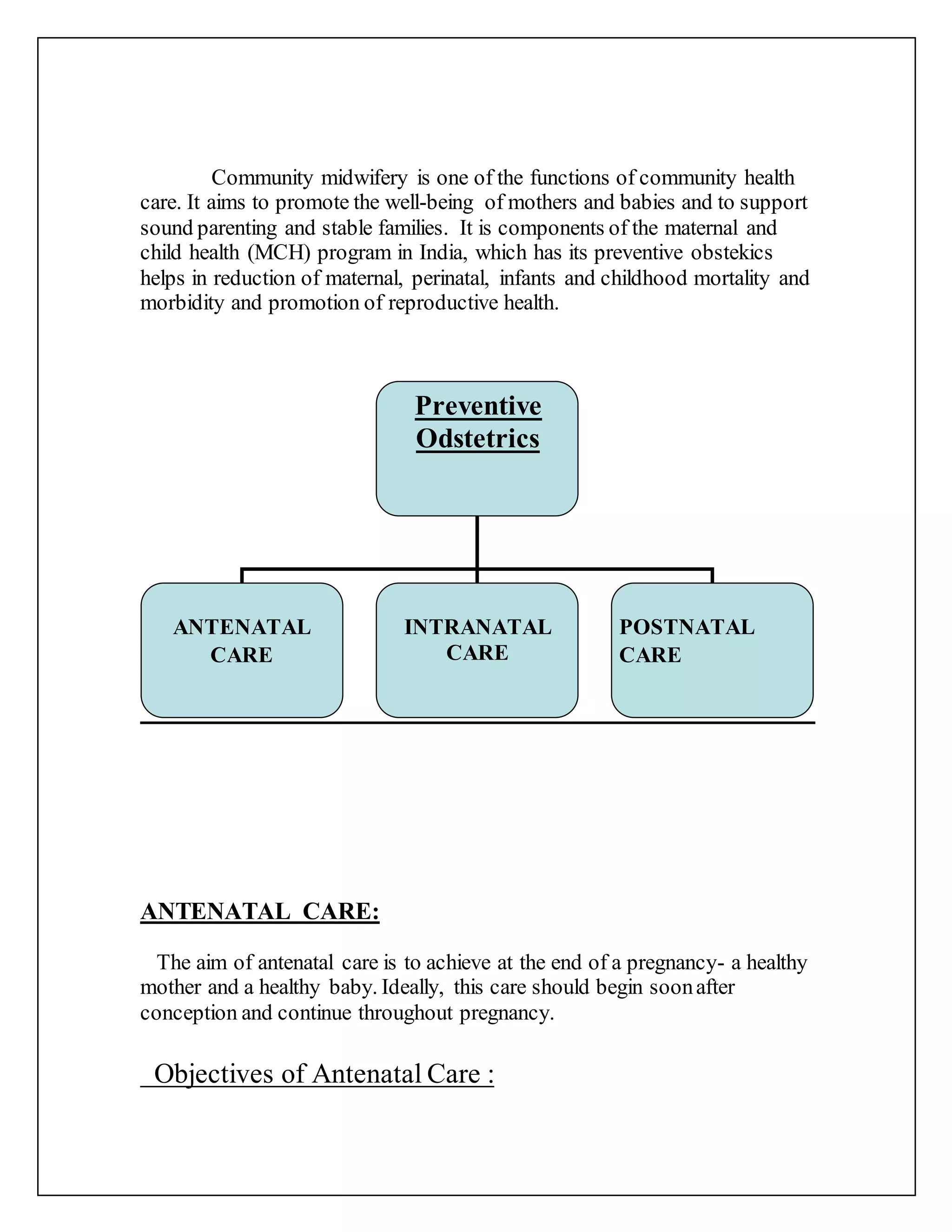







Community midwifery aims to promote maternal and child health through antenatal, intranatal, and postnatal care. Antenatal care includes regular checkups to monitor the health of the mother and baby, identify high-risk pregnancies, provide education on nutrition and hygiene, and begin postpartum family planning. Intranatal care focuses on a clean delivery to prevent infections. Postnatal care supports breastfeeding and family planning education while checking for postpartum complications over 10 days of visits. The overall goals are a healthy mother and baby as well as promoting reproductive health.




































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)












