Downloaded 206 times












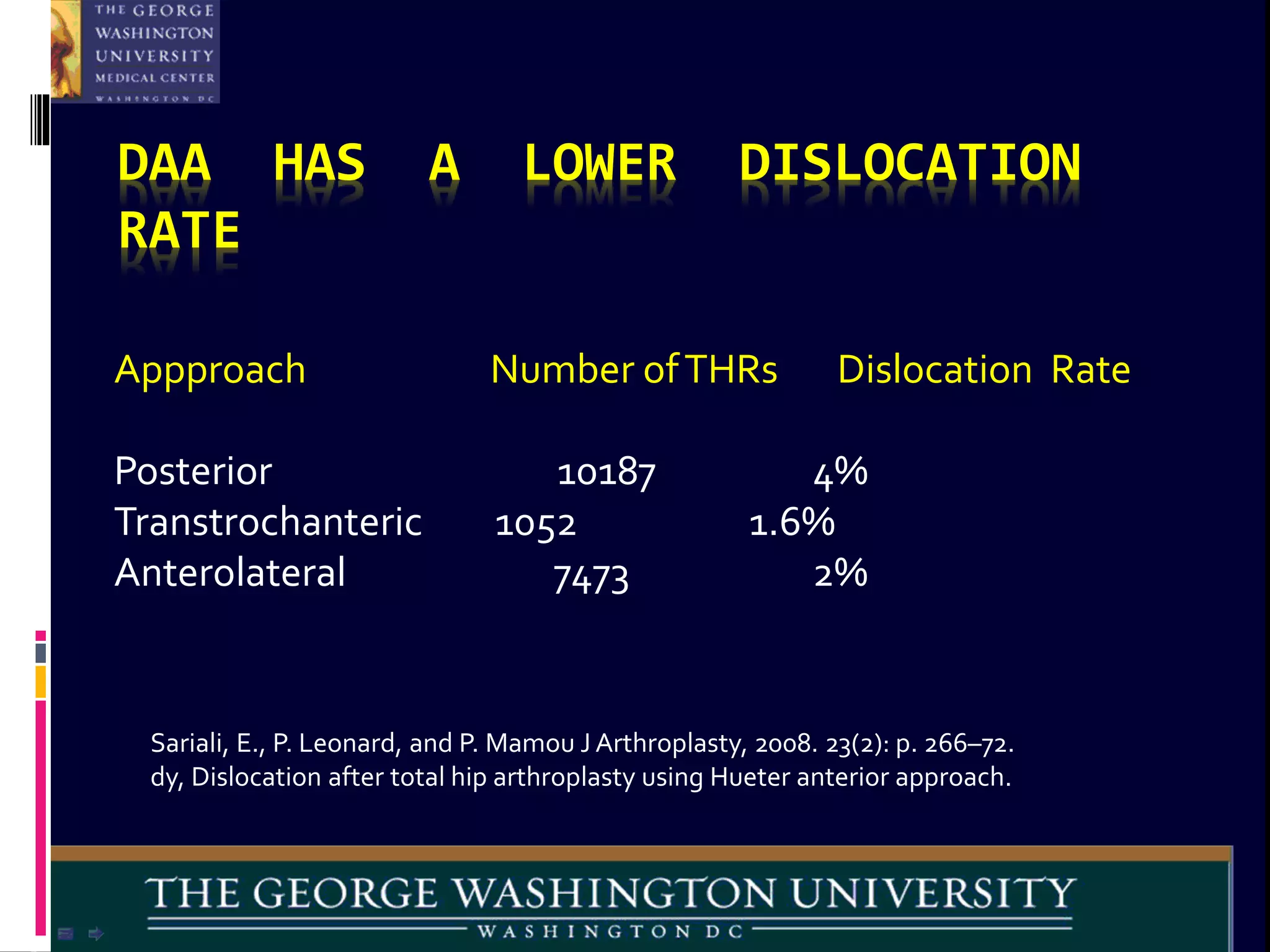


















The direct anterior approach (DAA) for hip replacement surgery has been described since the late 19th century but saw limited use until more recent decades. Proponents argue the DAA has advantages over other approaches like less soft tissue damage, faster recovery, and lower dislocation rates. Studies have found the DAA results in less muscle damage, lower inflammatory marker levels, and shorter hospital stays compared to posterior approaches. While specialized tables have been used, the DAA can also be performed on a standard operating table. Overall, the available evidence and experiences of surgeons indicate the DAA may offer benefits for patients undergoing hip replacement.











































































































